

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Cecal diverticulitis is a rare condition that was first described by Potier [1] in 1912. Right-sided colonic diverticulitis shows a higher prevalence in Oriental countries than in Western countries [2]. It is well known that its incidence is increasing with the growth of the elderly population [3]. Diverticulosis is a rare condition during gestation. Almost all the cases of cecal diverticulitis are found after exploration for suspected acute appendicitis because there is a close resemblance in clinical features between cecal diverticulitis and acute appendicitis. Pregnancy causes changes in the physiologic and anatomical findings of the gastrointestinal tract. This poses a diagnostic and therapeutic challenge for clinicians during pregnancy. With a rare presentation of cecal diverticulitis during pregnancy, there are no established protocols for the diagnosis and treatment of it. To date, an aggressive surgical intervention has been advocated to minimize the risk of maternal morbidity and fetal loss due to complications resulting from delayed diagnosis such as inflammation, perforation, and, hemorrhage [2]. We experienced a case of cecal diverticulitis during pregnancy and then successfully treated with postoperative antibiotic treatments without resection. Our case indicates that a patient with cecal diverticulitis during pregnancy could be medically managed. Here, we report our case with a review of literatures.
Case Report
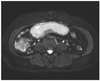
A 24-year-old, gravid 1, para 0, woman was referred to the emergency care center for further evaluation and treatment of the right lower quadrant (RLQ) pain at 19+1 weeks of gestational age. Three days prior to visit, the patient first experienced RLQ pain concurrently with nausea and four episodes of diarrhea. After then, the patient presented with an intermittent pain, cramping and getting more severe in nature. The patient had no notable past history and her pregnancy course was uneventful. The patient had a 1 pack-a-day smoking history, but quit smoking after pregnancy. On physical examination, the patient had a body temperature of 36.6℃, a gravid abdomen appropriate for the age of gestation and soft abdomen. There was a marked abdominal tenderness with positive rebound sign in the RLQ region. The results of clinical laboratory tests were all within the limits of normal range except for elevated white blood cell (WBC) counts of 10,900/µL. Compression ultrasound of the RLQ revealed a cecal wall thickening with a preserved stratification and an increased echo texture of the adjacent mesenteric fat. However, ultrasound did not demonstrate the structure of the appendix due to a poor sonic window. Magnetic resonance imaging (MRI) examination revealed a focal wall thickening of the cecum, terminal ileum and appendix with pericecal high intensity on T2 spectral adiabatic inversion recovery (SPAIR) fat suppressed sequence. These findings were interpreted as enterocolitis with secondary appendicitis (Fig. 1). These results of ultrasound and MRI led us to a provisional diagnosis of acute appendicitis. Then, the patient underwent emergency laparoscopy which revealed a solitary inflamed mass on the anterior wall of the cecum and a secondary inflammation of the appendix (Fig. 2). After a routine appendectomy, the diverticulitis was managed with intravenous antibiotic therapy (ampicillin/sulbactam 1.5 g every 12 hours and ornidazole 500 mg every 12 hours). On postoperative day 5, the patient was afebrile with a mild, localized pain in the right lower back. There were no notable findings on ultrasound of the fetus and the placenta. Besides, there was a lack of the uterine contraction. Clinical laboratory tests showed normal WBC counts except for an elevated C-reactive protein level of 95.25 mg/L. The treatment regimen was switched from ornidazole to cefoxitin (1 g every 8 hours) for further 5 days. The patient was advised to a low-fat, high-fiber diet for the prevention of the constipation. The patient remained afebrile. On follow-up laboratory tests showed that WBC counts were normal and C-reactive protein levels were decreased to 15.76 mg/L. The patient achieved an uneventful recovery and was discharged on postoperative day 10. On routine examination at the outpatient clinic, the patient did not complain of any notable symptoms except for a sustained presence of the mild pain in the right lower back. At 32 weeks and 0 day's gestation, the patient complained of night sweats. The patient was afebrile and had notable findings on fetal sonographic examination. The patient was therefore given regular follow-ups. At 35 weeks and 4 days' gestation, the patient presented with dyspepsia and acid regurgitation for three days and then hospitalized. The patient had a persistent presence of the right lower back pain and night sweats, but presented with no fever. Clinical laboratory tests showed that WBC counts were normal (8,710/µL) and C-reactive protein levels were slightly elevated (5.5 mg/L). This was followed by the initiation of antibiotic treatments (ampicillin/sulbactam 1.5 g every 8 hours). At 36 weeks and 0 day's gestation, a caesarean section was performed under the suspicion of recurrent attack of diverticulitis. A normal female infant weighing 2,740 g was born with Apgar scores of 9 and 10 at 1 and 5 minutes, respectively. Intraoperatively, there were inflammatory changes in the cecal wall and fibrotic adhesions between the cecal wall and omentum. It was difficult to identify the diverticulum under the gravid uterus and through a Pfannenstiel incision. We decided conservative management. The postpartum course was uneventful. The patient was discharged on postoperative day 5. Four weeks thereafter, the patient was fine without problem on an outpatient follow-up. Five months after discharge, the patient was asked any recurrent episodes through a telephone interview. The patient had no recurrent episodes.
Discussion
Right-sided diverticular disease is rare and it accounts for 1%-3.6% of total cases of colonic diverticulitis in western countries. In Asian series of patients, however, it is more commonly seen and accounts for approximately 43%-50% of total cases of colonic diverticulitis [2]. Right-sided diverticular disease occurs more frequently in younger patients and it shows a male predilection. But its left-sided counterpart is seen more commonly in the elderly and shows no sex-related difference [2]. The pathogenesis of diverticular disease remains uncertain. It is hypothesized, however, that its pathogenesis is complex and it is based on the interactions between the genetic factors and other various factors (colonic structure, intestinal motility and diet) as well as all of these individual factors [4]. Most cases of right-sided diverticular disease are asymptomatic. Symptoms occur only when it is complicated by inflammation, bleeding, or perforation [5]. Its pathophysiology remains unclear. In our case, the patient was a heavy smoker (more than 10 cigarettes/day), but quit smoking after pregnancy. A population-based prospective study of Swedish women demonstrated that smoking was associated with symptomatic diverticular disease and the risk of complications was almost doubled among current smokers compared with non-smokers [6].
It may be difficult to make a differential diagnosis of cecal diverticulitis from acute appendicitis. More than 70% of patients with cecal diverticulitis are surgically treated under a clinical diagnosis of acute appendicitis [7,8].
Diverticulitis of any colonic part complicating pregnancy is a very rare occurrence. To date, only three single case reports discuss this coincidence. Therefore, it may often be impossible to make a diagnosis of cecal diverticulitis in pregnant women. Anatomic and physiologic changes during pregnancy often mask and delay the diagnosis. This explains a higher rate of perforation and subsequent complications of cecal diverticulitis during pregnancy. Abdominal ultrasound is widely used as the first-line diagnostic modality in pregnant women presenting with acute abdomen because of its non-invasiveness and rapid availability. However, ultrasonography during pregnancy is often inconclusive.
An MRI is an accurate imaging modality for the diagnosis of acute abdominal and pelvic pain during pregnancy and it should be considered in patients with an inconclusive ultrasound [9]. Despite the advances in these imaging techniques, most of patients are intraoperatively diagnosed with diverticulitis at a diagnostic accuracy of 65%-85% [10].
The treatment regimen for patients with cecal diverticulitis includes antibiotics therapy with supportive management and surgical intervention. It is suggested that conservative management with broad spectrum antibiotics be used for patients who were preoperatively diagnosed with cecal diverticulitis [5]. There is a considerable controversy regarding treatment regimen for patients who were diagnosed with cecal diverticulitis during laparotomy. If diagnosed intra-operatively, postoperative antibiotic therapy after routine appendectomy leaving diverticulum in situ has been advocated for uncomplicated diverticulitis [7]. There is a possibility, however, that an inflammatory cecal carcinoma might be missed during the conservative managements with antibiotics [5,8]. When confronted with multiple diverticuli and cecal phlegmon, or when neoplastic disease could not be completely ruled out, an immediate right hemicolectomy is advocated [7]. Fang et al. [11] recommended an aggressive surgical resection of cecal diverticulitis. Because less than 40% of patients were successfully treated with conservative methods. They also reported that there was a recurrence of diverticulitis in 29% of patients who received only appendectomy, a later right hemicolectomy was needed in 12.5% of them.
However, there are recent trends toward either conservative or less invasive management of diverticulitis. According to the American Society of Colon and Rectal Surgeons, up to 80% of patients with acute diverticulitis are treated with conservative therapy, and approximately 85% of these successfully avoid an emergent or urgent operation [12,13]. Approximately one third of patients have no second attack, and only another one third have reported a recurrence of diverticulitis, leading to an overall readmission rate of 2% per year for diverticulitis. It might therefore be reasonable, with appropriate patient education, operation may be avoided in selected patients [13]. In addition, the prospective data provide evidence that intake of high-fiber diet is effective in not only preventing the occurrence of diverticular disease but also lowering the incidence of symptomatic diverticular disease [14]. However, there is no consensus on the diagnosis and treatment of cecal diverticulitis in pregnant women because it is an extremely rare entity. In our case, the patient received a combination therapy with antibiotics after appendectomy without a resection of the lesion. This was followed by the modification of eating habit and lifestyle. Our case indicates that the conservative management could be considered as an adequate approach in pregnant women with non-perforated cecal diverticulitis. It is important to emphasize, however, that they should be considered highly selected cases and their clinical course meticulously monitored to detect the complications. If refractory to the conservative treatments, they would be in need of aggressive intervention to minimize the risks to the mother and fetus.
In conclusion, our case indicates that clinicians should consider cecal diverticulitis as one of possible causes of acute abdomen in pregnant women.

 XML Download
XML Download