

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Menopause is defined as the absence of natural menstruation for more than 1 year and is an important marker of endocrine and reproductive changes in women; this condition refers to permanent loss of fertility. The basic change observed in this reproductive senescence is depletion of oocytes in the ovaries, and these changes occur over a wide age range (40 to 60 years) [1] rather than at a definite time point. This period is a dynamic transition with respect to clinical and endocrine changes. The Stages of Reproductive Aging Workshop (STRAW) classification system is now widely used for categorizing the menopausal transition period, according to the study by Soules et al. [2].
While the mean age of menopause is reported worldwide to be 51 years, there are few markers to predict when menopause will occur in individuals, because the reproductive endocrine changes that occur during this transition period are inconsistent and variable. An estimation of menopause or the menopausal transition period is important for clinicians for appropriate management of menopausal symptoms and hormone therapy (HT)-related side effects. In addition, the timing of HT initiation might be the main factor determining the cardiovascular protective effect of HT [3-5], thus emphasizing the importance of this prediction.
The level of serum follicle-stimulating hormone (FSH) has traditionally been used as a marker of ovarian reserve, but it is limited by large cycle-to-cycle variation, requiring repetitive measurements to be applied clinically. In some cases, it is not as powerful as the last menstrual period for predicting menopause (or the final menstrual period) [6,7].
Recently, anti-Müllerian hormone (AMH), also known as Müllerian-inhibiting substance [5], which is a member of the transforming growth factor-β superfamily, has received attention in the reproductive endocrinology field. AMH may be a marker for ovarian responsiveness in controlled ovarian-stimulation cycles [8-10]; it is considered to be a reliable ovarian reserve marker because it is produced only from the ovary, and its levels constantly decrease with age [11,12]. Furthermore, AMH is undetectable in women after spontaneous or surgically induced menopause [13]. Many studies have reported AMH levels as a promising predictor for the occurrence of menopausal transition or menopause [14-16].
Ultrasonographically assessed antral follicle count (AFC) and ovarian volume have also been suggested as sensitive and specific markers of ovarian aging and menopause [17-19] because the number of total follicles is regarded as a good indicator of the remaining primordial follicle pool size, which decreases with age since sonographic markers reflect the endocrine status [20-22].
The objectives of this study were to evaluate the usefulness of measuring serum AMH levels for predicting menopause in women who have already entered their menopausal transition period over a relatively short period of 1 to 2 years. In addition, we assessed serum levels of FSH, estradiol, AFC, endometrial thickness (EMT), days from the last menstrual period (LMP), and interval of LMP from the previous cycle as markers for predicting menopause in late reproductive-aged women.
Materials and Methods
1. Study population
A cohort of 104 women, aged 45 to 55 years (mean age 49.7 ± 2.3 years), who were predicted to be in their menopausal transition (previous regular cycles with changes in their menstruation in the previous 6 months) were selected from a group of women who visited Seoul National University Gangnam Center more than twice for an annual routine health check-up between September 2008 and March 2011.
The inclusion criteria were as follows: 1) 45- to 55-year-old premenopausal women having an intact uterus and both ovaries; 2) proven fertility: more than 1 live birth; and 3) previous regular menstrual cycles of 21 to 35 days with a change in cycle in the previous 6 months (shortening or lengthening of their cycle for more than 7 days). The exclusion criteria were as follows: 1) history of hysterectomy or ovarian surgery; 2) large-sized myoma, adenomyosis with endometrial distortion, or ovarian tumor examined by ultrasonography; 3) chronic debilitating diseases such as malignancies, thyroid, or renal diseases; 4) use of oral contraceptive pills; or 5) current smokers.
Participants were assessed twice (T1 and T2) at a mean interval of 13.1 months (range, 6 to 30 months). At each time, their menstrual history (LMP, previous menstrual period) was assessed by a medical interview at the time of their routine gynecologic examination. Pelvic ultrasonography was performed to evaluate AFC and EMT; blood samples were obtained to assess serum levels of AMH, FSH, and estradiol. Reproductive characteristics such as age at menarche and parity were recorded during a medical interview using a structured questionnaire and verbal confirmation during routine gynecologic examination.
Most of the participants voluntarily paid for their health checkups; some women were supported by their employer or by their spouses. This study was approved by the Institutional Review Board of Seoul National University Hospital.
2. Methods
1) Classification of menopausal transition status
Menopausal transition status was classified according to the STRAW system. At T1, participants were in either EMT or LMT.
(1) Early menopausal transition (EMT): variable-length cycles with more than 7 days of difference from normal.
(2) LMT: 2 or more skipped menstrual cycles and at least 1 intermenstrual interval of 60 days or more.
(3) Menopause: amenorrhea for more than 12 consecutive months.
2) Blood samples and hormonal measurements in serum
Blood samples were obtained from the participants after they were subjected to overnight fasting. Samples were obtained from all participants at T1, but from only 62 participants at T2. Serum samples were stored at -20℃ until assayed. AMH concentrations were measured from all serum samples by using an enzyme-linked immunosorbent assay (ELISA, Immunotech, Marseille, France). Intra- and inter-assay coefficients of variation were 12.3% and 14.2%, respectively, with a detection limit of 0.14 ng/mL. Serum FSH and estradiol were assayed using an immunoradiometric assay [23] and radioimmunoassay [24], respectively (Siemens, Los Angeles, CA, USA). For FSH, the sensitivity of the test was 0.06 IU/L, with intra- and inter-assay coefficients of variation of 3.8% and 5.7%, respectively. For estradiol, the sensitivity of the test was 8 pg/mL, with intra- and inter-assay coefficients of variation of 7% and 8.1%, respectively.
3. Ultrasonographic evaluation
All participants received transvaginal or transrectal ultrasonography to assess for AFC, EMT, or any pathologic findings in the pelvis by using a 5.5 MHz probe (GE, Seoul, Korea). The examination was performed on the participant's visiting day for health checkup it was irrespective of menstrual cycle.
4. Statistical analyses
The continuous variables measured in this study were expressed using mean and standard deviation (SD) values. We used Fisher's exact test to determine if the frequency of menopause was different between groups with detectable and undetectable AMH levels. To analyze the change in values between each visit, the paired t-test, Wilcoxon signed-rank test, and McNemar's test were used. Pearson's correlation analysis was used to determine whether a correlation existed between the reproductive characteristics and hormonal levels.
A logistic regression analysis with the outcome measure as occurrence of menopause at T2 was performed to identify the most predictive marker of menopause. The area under the receiver operating curve (ROCAUC) was calculated as a measure of predictive accuracy.
All statistical analyses were performed using the SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA). A 2-tailed P-value<0.05 was considered statistically significant.
Results
1. Characteristics of the study population at T1 and menopausal status at T2
The mean age of the 104 enrolled participants was 49.7 ± 2.3 years (range, 45 to 55 years). Of these, 20 were in EMT, and 84 were in LMT; 17 of 20 women (85.0%) in EMT and 73 of 84 women (86.9%) in LMT had non-detectable AMH levels. By comparison, only 1 of 20 women (5.0%) in EMT and 32 of 84 women (38.1%) in LMT were menopausal at T2 (P = 0.004) (Table 1).
2. Characteristics of the study population at T1 according to menopausal status at T2
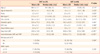
When the participants were grouped according to their menopausal status at T2 (non-menopausal women at T2, n = 71, vs. menopausal women at T2, n = 33), the menopausal group had higher FSH, longer number of days from LMP and interval days between their last 2 cycles, and lower values of estradiol, EMT, and AFC. In contrast, no difference was observed in AMH values between the groups, and most participants had non-detectable levels of AMH (85.9% and 87.9% for the non-menopausal and menopausal groups, respectively) (Table 2).
3. Changes in hormonal, ultrasonographic, and clinical markers at each visit
All participants visited at both T1 and T2; blood samples were obtained from all participants at T1, but blood samples for hormonal assays were obtained from only 62 women at T2. When the paired values were compared between the 2 times, levels of estradiol, EMT, and AFC were significantly decreased, and menstrual cycle days became much longer at T2. For AMH levels, 25.9% of the participants that had undetectable levels at T1 had detectable levels of AMH at T2 (Table 3).
4. Correlation among ovarian reserve markers
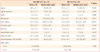
The correlation analyses after adjustment for age revealed that FSH levels were negatively correlated with estradiol, EMT, and AFC and were positively correlated with days from LMP. EMT was positively correlated with estradiol levels and was negatively correlated with prolonged days after the last menstrual cycle and previous menstruation. AFC was also negatively correlated with the number of days since LMP (Table 4).
5. Predictive capacity of ovarian reserve markers and menstrual history assessed at T1 for menopause at T2
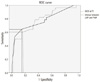
The results of univariable logistic regression analysis are presented in Table 5. Among the hormonal and sonographic markers, lower levels of FSH and higher values of estradiol, EMT, and AFC at T1 were associated with a lower probability of menopause at T2. A longer number of days after LMP and a larger gap between the last 2 cycles were significantly associated with the onset of menopause at T2. Detectable values (>0.14 ng/mL) of AMH at T1 did not show significant correlation with menopause at T2. In the multivariable stepwise logistic analysis, the variables of days since LMP and interval between LMP and the previous menstrual period (PMP) were selected as independent risk factors for predicting menopause in our model (Table 5). When 60 days (2 months) was selected as the cutoff, the sensitivity was 60.1%, and the specificity was 81.5% for the number of days since LMP; for the interval between the last 2 menstrual cycles, the sensitivity for predicting menopause at T2 was 64.3%; specificity was 84.6% with 75 days (2.5 months) as the cutoff (Fig. 1).
Discussion
Our study included women who were more than 45 years of age and were in their late reproductive years with irregular menstruation; serum levels of AMH were undetectable in most cases (86.6% at T1, 74.2% at T2), and detectable values of AMH were not associated with menopause over a 13-month period. In addition, the mean AMH value did not decrease over time. However, 15 of 58 women (25.9%) with undetectable levels of AMH at T1 showed detectable serum levels of AMH at T2. These results were unexpected because we had hypothesized a linear decrease in AMH levels over time and that AMH levels at T1 would be a predicting factor of menopause at T2.
A number of recent studies have suggested that AMH is a promising marker for predicting the menopausal transition or menopause [14-16,19]. In contrast to our study, the target population in other studies included young, reproductive-aged women (25 to 46 years old or 40 to 50 years old), and the follow-up interval spanned a longer period (6 to 11 years).
Serum AMH levels have been reported to be constant throughout the natural menstrual cycle in young, reproductive-aged women; therefore, AMH levels have been regarded as a reliable serum marker of ovarian reserve that can be measured anytime during the menstrual cycle, at the convenience of clinicians [25-29]. However, Robertson et al. [29] reported recently that AMH levels could change significantly throughout the ovulation cycle in late reproductive-aged women (>45 years old); some women had a 2.8-fold increase, while others had a 4.3-fold decrease in levels in the luteal phase compared with those observed in the follicular phase. Furthermore, 19% of the women had non-detectable levels of AMH during their ovulation cycle based on other hormonal assays even though the sensitivity of their assay was 10-fold higher than the assay used in our study (0.017 ng/mL). Therefore, the authors concluded that AMH levels become less reliable as a marker of ovarian reserve when levels are substantially reduced, as in late reproductive-aged women [29]. Likewise, there have been reports of moderate and reasonable pregnancy rates following extremely low levels of serum AMH in women in vitro fertilization programs [30].
Although we did not monitor intracyclic fluctuations of AMH levels because we did not measure blood progesterone levels, and blood samples were taken irrespective of the menstrual cycle, we found that 25.8% (all participants with detectable levels of AMH at T2 had lower or undetectable levels of AMH at T1) of participants had higher serum values of AMH after 13 months, which might be due to an unpredictable abrupt change that occurs in women at a late-reproductive age. Elevated basal FSH level, decreased AFC (or ovarian reserve), and the resulting unpredictable ovarian response, are thought to be important markers, but more studies are needed to further understand the underlying ovarian physiology at this age. As expected, FSH-the classical marker of ovarian aging-and AFC-the well-established sonographic marker of ovarian reserve-were significantly associated with predicting menopause as a single marker in our study. However, hormonal and sonographic markers including FSH and AFC were not significantly associated with development of menopause after multiple stepwise regression analyses. Instead, a longer interval from their LMP and a larger gap between their last 2 cycles in late reproductive-aged women were most strongly and independently associated with occurrence of menopause after 1 year in women who had already entered the late reproductive period in our study.
There were some limitations in this study. First, there is a possibility of recall bias because the information regarding the LMP was retrospectively obtained from the participants. Second, at T2, blood samples were obtained from only 62 of the 104 participants due to a lack of remaining blood samples after the routine blood examination. A larger study group may be required. Third, since it has been known that the endocrine status of EMT and LMT is different, recruitment of adequate number of participant of each state at T1 (especially subjects in EMT) could have given more detailed information. In addition, the AMH ELISA kit used in this study was not sensitive enough to discriminate differences in very small antral follicle numbers. Only 14 of 104 participants (13.4%) at T1 and 16 of 62 (25.4%) at T2 had detectable levels of AMH. Accordingly, any statistical analysis that could reveal a quantitative association among other hormonal or sonographic markers with AMH was not possible. Development and application of a more sensitive tool is required for future studies. Furthermore, any study design that investigates the level of AMH to predict menopause would better span longer period to cover reproductively younger women that might have measurable AMH level.
Nonetheless, despite the small study group size, this is the first longitudinal Korean study that evaluates the usefulness of AMH, other hormonal and ultrasonographic markers, and menstrual history as markers for predicting menopause in a relatively short timeframe in late reproductive-aged women. These data can be obtained during a routine gynecologic examination where information regarding the exact timing of menopause and hormonal status is important to both the clinician and the examinee. Women who have not menstruated for more than 2 months and who are 45 to 55 years old have a high probability of becoming menopausal after 1 year without requiring further hormone evaluation. This study indicates that AMH is not a determining marker for predicting the onset of menopause in late reproductive-aged women in a relatively short timeframe (range, 0.5 to 2.5 years). The traditional ovarian reserve markers FSH and AFC were not independent predictors, but time since the LMP and longer intervals between the last 2 cycles at T1 were more useful predictors of menopause onset.
Serum values of AMH in this age group of women were very low and changed sporadically; hence, a more sensitive assay kit should be used, and ovulation cycle timing should be a consideration.




 XML Download
XML Download