

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Choriocarcinoma is one of gestational trophoblastic tumor. Metastases from gestational trophoblastic tumor (GTT) occur most commonly in lung, vagina, central nervous system, liver and gastrointestinal tract. In this case report we describe a rare case of metastatic choriocarcinoma which presented with acute right flank pain due to kidney rupture secondary to a renal metastasis.
Case Report
A 33-year-old female presented to emergency department with a complaint of acute right flank pain. She gave a past history of dilatation and curettage (D&C) after an episode of spontaneous abortion. Due to persistent vaginal bleeding after the procedure she had been treated with 2 cycles of methotrexate at local clinic center under the impression of gestational trophoblastic disease (GTD). And yet, vaginal spotting continued. She came to our gyneco-oncology department in August, 2010 with beta-human chorionic gonadotropin (β-hCG) level of 140. Biopsy results from D&C showed decidualized endometrium with congestion; however, laparoscopically vaginal hysterectomy was done to rule out GTT. Biopsy results from laparoscopic assisted vaginal hysterectomy (LAVH) confirmed choriocarcinoma. Postoperative β-hCG level was decreased to 21. It decreased to less than 2.0 after first cycle of chemotherapy then it maintained fewer than 2.0. Three cycles of chemotherapy with etoposide, methotrexate, actinomycin D, cyclophosphamide and vincristine was followed until the patient attains three consecutive undetectable hCG levels. Monthly follow-up of β-hCG was done for 5 months. On abdomen and pelvic computed tomography (CT) after completion chemotherapy, we confirmed there was no evidence of remnant mass in abdomen.
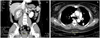
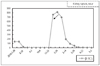
After 5 months from last chemotherapy she presented to our emergency department with a complaint of sudden onset of right flank pain. A vaginal examination of pelvis was normal. The CT scan showed a large renal hematoma including a hypervascular mass with active bleeding which implied right kidney rupture and multiple organ metastases of liver and lung including multiple mass in right kidney with active bleeding which implied kidney rupture (Fig. 1). At this time β-hCG level was increased up to 756 (Fig. 2). A decision to undertake angioembolization of the renal masses was taken and angiography was performed, which revealed a large hypervascular right renal mass and areas of contrast pudding within the renal mass (Fig. 3). Emergency embolization was performed using 5×50-mm steel coil (Cook, Bloomington, IN, USA) in order to become hemodynamically stable as a result of stop further bleeding. After the procedure the patient had a mild fever and flank pain, which were controlled with antipyretics and analgesics. As the patient was becoming hemodynamically stable, the patient was started on an additional chemotherapy with cisplatin, etoposide, actinomycin D, methotrexate. The patient was alive and well when last seen, 13 months after presentation.
Discussion
Choriocarcinoma is a highly malignant neoplasm of trophoblastic cells in young women of childbearing age. Women who are sexually active are at risk for developing GTD, with a higher incidence before 20 and after 40 years [1]. Hematogenous metastases in a choriocarcinoma widely disseminate to lungs, vagina, brain and liver. Renal metastasis from choriocarcinoma is extremely rare and only few reports have been published. The incidence of renal metastasis at autopsy varies from 1.8% to 11.8% [2]. Choriocarcinoma being a vascular and hemorrhagic tumor has a propensity to rupture especially when in subcapsular location due to direct pressure of increased intravascular pressure secondary to tumor emboli, resulting in intra-renal venous obstruction [3]. Spontaneous renal hemorrhage is a difficult to diagnose due to variety of causes. However in case of spontaneous renal hemorrhage in women of child-bearing age, metastatic choriocarcinoma should be considered as one of the differential diagnosis. And serum hCG level should be evaluation to confirm the diagnosis.
In our case, CT was probably performed earlier in the development of the lesion and thus showed a profuse vascular pattern. Biphasic CT imaging shows the lesions to be hypervascular in arterial phase with washout in renal venous phase. Renal metastases have also been described as avascular lesions [4], which could be caused by extensive hemorrhage leading to necrosis of an initially vascular lesion. Unlike most malignant tumors, choriocarcinoma is unique in that its diagnosis and management is based more upon the β-hCG levels rather than upon the histopathological diagnosis. Although imaging studies can alert the physician to its possible diagnosis in cases of early disease, the principal role of imaging is in the detection and staging of metastatic disease.
Treatment of spontaneous rupture of choriocarcinoma metastasis of kidney is decided at the tumor size, tumor location, and severity of bleeding [5]. Surgery is usually difficult in this case, because of hemodynamic instability. Percutaneous transcatheter embolization (PTE) offers an alternative treatment to surgery [6]. In our case, the angiography used detection of the renal metastasis to be hypervascular lesion with a tumor which was embolised to stop bleeding. Steel coils were used in embolization to occlude the vessels and stop further bleeding. PTE should be selected to control the bleeding in these cases because surgical resection is not curative. It is an effective and fast procedure which can stop bleeding in a short period of time and control hypotension, hypovolemic shock or death. The bleeding vessel is identified with angiography and selectively embolized with immediate confirmation of the result. Since embolization can be performed under local anesthesia and mild sedation unstable patients do not have to undergo extensive surgery. The procedure is quick and safe way to stabilize life threatening condition with rare complication. Besides control of hemorrhage, emoblization has been suggested for preoperative reduction of tumor vascularity, and therapeutic reduction of tumor bulk.
After embolization proper chemotherapy with combination regimen should be considered. The patient should receive follow up with weekly measurement of β-hCG level until they are normal for 3 consecutive weeks and monthly measurement for 12 consecutive months.
This case report is significantly meaningful because presentation of metastastic choriocarcinoma in kidney is rare with the advent of highly effective chemotherapy. And this report showed great use of embolization for gynecologic emergency. Because embolization has been usually used for obstetric-related hemorrhage and studies about hemorrhage in gynecologic condition is rare.

 XML Download
XML Download