

 PDF
PDF ePub
ePub Citation
Citation Print
Print


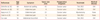
Uterine lipoleiomyoma is a rare benign lesion accounting for 2.1% of all leiomyomas and is composed of mature adipose tissue and smooth muscle cells [1-3]. Although the pathogenesis of the lipoleiomyoma is unclear, immunohistochemical studies reveal that lipoleiomyoma may arise from metaplasia of pluripotent mesenchymal cells or direct metaplasia of smooth muscle cells [4]. Also there are reports that uterine lipoleiomyoma may associate with certain metabolic disturbance including diabetes mellitus or hyperlipidemia [5,6]. We found only six cases of lipoleiomyoma of the broad ligament through an English literature review [1,7-10]. Lipoleiomyoma of the broad ligament is frequently diagnosed at the time of surgery due to its similarity to ovarian tumor (Table 1).
Case Report
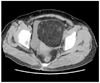
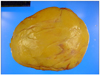
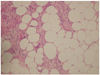
A 56-year-old multiparous menopausal woman was admitted to our hospital due to pelvic mass and lower abdominal discomfort for 3 months. She had menopause 3 years ago and body mass index of 24.7 kg/m2. Pelvic examination demonstrated gestational age 20 weeks sized, movable hard mass in the pelvis. Pelvic ultrasonography revealed 15×15 cm sized heteroehoic left adnexal mass (Fig. 1). Laboratory test showed hyperglycemia (282 mg/dL; normal range, below 200 mg/dL), elevated hemoglobin A1c (6.5%; normal range, 4.4%-6.3%). Cholesterol, triglyceride and tumor markers (CA-125, CA 19-9, carcino embryonic antigen, alpha fetoprotein, beta-human chorionic gonadotropin) were within normal limits. Contrast-enhanced computed tomography showed a 15×14 cm sized left adnexal tumor with low-attenuated fatty tissue (Fig. 2). Preoperative diagnosis of ovarian mature cystic teratoma was made. However we could not exclude the possibility of degenerative uterine myoma. We decided exploratory laparotomy. During the surgery, we found a 15 cm-sized retroperitoneal tumor that protrude into the abdominal cavity. The connection between the tumor and the left ovary did not exist. The tumor attached to the left lateral aspect of the uterus. Tentative diagnosis of intraligamentary myoma with degeneration was made. We performed total abdominal hysterectomy with bilateral adnexectomy. Gross findings of the resected tumor showed homogeneous, yellow color and smooth surface contour (Fig. 3). The tumor measured 19 × 13 × 7.5 cm and 940 g in weight. Microscopically, the tumor showed proliferation of mature fat tissue with scattered smooth muscle bundles without cellular atypia and vascular proliferation (Fig. 4). No specific findings were seen in the both adnexa, cervix, myometrium and endometrium. The final diagnosis was lipoleiomyoma of the uterus. The patient discharged 7 days after surgery without complication and was free of the tumor 3 months after surgery.
Discussion
Uterine lipoleiomyoma is composed of mature fat tissue and smooth muscle cells. Uterine lipomatous tumors are classified in three groups: 1) pure lipomas, which are composed of mature adipose tissue and well encapsulated, 2) lipoleiomyomas, which are composed of various amount of mature adipose tissue and smooth muscle cells, and 3) the rarest malignant tumors, which have cellular atypia [1]. Traditionally, there are two hypotheses for the pathogenesis of uterine lipoleiomyoma [1,4]. The first is that lipoleiomyoma arises from direct metaplasia of the smooth muscle cells of leiomyoma. The second is that lipoleiomyoma arises from metaplasia of pluripotent mesenchymal cells. Rare lipoleiomyoma with renal angiomyolipoma-like vascular proliferation have been reported [11]. In our case, microscopic findings did not show cellular atypia and vascular proliferation. In the view of direct metaplasia of the smooth muscle cell, lipoleiomyoma can be associated with metabolic disorders including diabetes mellitus and hyperlipidemia because plasma lipids can offer a source for the fat deposition of smooth muscle cells [5,6]. Also many lipid metabolism disorders are originated from postmenopausal estrogen deficiency and promote the abnormal intracellular storage of lipids. These may explain the fact that uterine lipoleiomyomas are mostly seen in postmenopausal women. The present case revealed hyperglycemia, elevated hemoglobin A1c and normal range of cholesterol and triglyceride. The differential diagnosis of uterine lipoleiomyoma includes ovarian or retroperitoneal mature cystic teratoma, benign lipoma, liposarcoma and angiomyolipoma [11,12]. Clinical symptom of lipoleiomyoma is similar to that of leiomyoma. Many patients remain asymptomatic and unrecognized [4]. Our patient had also vague abdominal discomfort for 3 months. Radiologic diagnosis of lipoleiomyomas with intraligamentary location can be difficult because of their similarity to ovarian tumors [9,10]. The fatty tissue of lipoleiomyoma produces the hyperechogenic area on ultrasonography, which is often misdiagnosed as a ovarian mature cystic teratoma. In our case, pelvic examination revealed huge pelvic mass with hard consistency similar to uterine myoma. However ultrasonography and computed tomography finding showed pelvic mass separate from the uterus and were similar to ovarian mature cystic teratoma. In conclusion, uterine lipoleiomyoma is rare benign disease. Differential diagnoses include ovarian mature cystic teratoma, degenerative leiomyoma and uterine sarcoma [4,13]. Accurate preoperative diagnosis of pedunculated intraligamentary lipoleiomyomas can be difficult due to their similarity to ovarian tumors.

 XML Download
XML Download