

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Preterm birth (PTB) is defined as birth before 37 completed weeks of gestation, which occurs in approximately 10% of all pregnancies [1]. PTB causes about 70% of all neonatal deaths of non-anomalous infants, as well as neonatal morbidities including respiratory distress syndrome, intraventricular hemorrhage, necrotizing enterocolitis, bronchopulmonary dysplasia and long-term complications such as cerebral palsy [2,3]. The PTB rate has risen worldwide, and in South Korea, the PTB rate has also risen from 4.3% in 1995 to 10% in 2003 [1,4].
There are many known risk factors for PTB, but one of the most important factors is previous history of PTB [1]. As mentioned before, global incidence of PTB rate is approximately 10%, but the rate of PTB increases up to 20%-50% in women with history of PTB, and the risk of PTB increases considerably with the number of previous PTBs [5-8].
For more than 30 years, progesterone administration has been advocated for the prevention of PTB in women considered to be at high risk for PTB [9]. However, the results of the earlier studies on the efficacy and safety of this treatment were controversial [10]. In 2004, two randomized controlled trials suggested that the prophylactic administration of progesterone in pregnant women at high risk for PTB, including those with prior history of PTB, is associated with a reduction of 60% to 78% in PTB rate [11,12]. After on, several randomized controlled trials reported that the use of progesterone reduced the risk of recurrent PTB [13-19]. In 2008, the American College of Obstetricians and Gynecologist published a committee opinion recommending the use of progesterone supplementation to prevent recurrent PTB in women with a singleton pregnancy and a prior spontaneous PTB due to spontaneous preterm labor or premature rupture of membranes [20].
However, the efficacy of the progesterone supplement therapy during pregnancy to prevent a recurrent PTB has never been studied in Korea. Therefore, primary objective of this retrospective study was to evaluate whether the prophylactic administration of vaginal micronized progesterone is associated with the reduction of recurrent PTB risk in women with a prior history of spontaneous PTB in Korean women.
Materials and Methods
We retrospectively evaluated the obstetric and neonatal outcomes of all women with history of one or more previous spontaneous PTB that delivered from January 2008 to April 2012. Spontaneous PTB was defined as PTB before 37 weeks of gestation due to spontaneous preterm labor or preterm premature rupture of membranes (PPROM). The exclusion criteria were multiple gestations either previous or current pregnancy, cerclage during both previous or current pregnancy, and previous intentional PTB due to maternal or fetal indications, such as preeclampsia and fetal growth restriction.
Patients who used progesterone were instructed to self-administer vaginal micronized natural progesterone (Utrogestan, Besins Healthcare, Brussels, Belgium or Yenatron, Acraf S.p.A., Roma, Italy) 100 or 200 mg capsule. The treatment was initiated at 16 weeks of gestation or at first visit to our hospital beyond 16 weeks of gestation. The treatment was continued until either 34 to 37 completed weeks of gestation or occurrence of PTB.
Control group consisted of singleton pregnant women with history of one or more previous spontaneous PTB and delivered in our hospital during the same study period, but who never used progesterone during current pregnancy. Patient selection, the dose of progesterone and the time of initiation and duration of the treatment were decided by the physicians' discretion.
Information of the previous pregnancy outcome such as number of previous term birth, number of previous PTB, gestational age and indication of the previous PTB was collected. Obstetric outcome of the current pregnancy including the rate of recurrent PTB before 34 weeks and 37 weeks of gestation of the two groups was compared.
The Fisher's exact test or Pearson's chi-square test was used for categorical variables. The Student's T-test or Mann-Whitney U test was used for continuous variables. The relationship between the incidence of PTB and independent variables including the number of previous PTB history, gestational age at previous PTB, indications of previous PTB and midtrimester cervical length were analyzed by multiple logistic regression analysis. A P-value of less than 0.05 was considered statistically significant.
Results
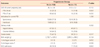
A total of 231 women were included in the study: 73 in the progesterone group and 158 in the non-user group. There were no significant differences in maternal characteristics including number of previous term and preterm births, and gestational age at previous PTB between the non-user group and progesterone group (Table 1). But there were more PPROM of indication for previous PTB in the progesterone group compared to the non-user group. Although mean cervical length during midtrimester ultrasound was not significantly different between two groups, more women in the progesterone group had cervical length less than 25 mm.
The incidence of recurrent PTB before 37 weeks of gestation was significantly lower in the progesterone group than the non-user group (21.9% vs. 43.0%, P=0.002) (Table 2). However, the rate of recurrent PTB before 34 weeks of gestation was similar in the two groups. There were no significant differences in other outcomes such as delivery mode, birth weight, 1-minute and 5-minute Apgar scores, and admission to neonatal intensive care unit.
Relationship between the incidence of PTB and independent variables were analyzed by multiple logistic regression analysis (Table 3). Midtrimester cervical length was significantly associated with the risk of recurrent PTB (odds ratio [OR], 0.916; 95% confidence interval [CI], 0.879-0.955). Use of progesterone was associated with significant reduction in recurrent PTB (OR, 0.382; 95% CI, 0.169-0.863).
We compared the characteristics and outcome of women who were treated with progesterone and delivered at term and those who delivered at preterm despite progesterone therapy (Table 4). Women who were treated with progesterone and delivered at preterm were more likely to have two or more previous PTB history compared to those who were treated with progesterone and delivered at term. Gestational age of previous PTB, number of previous term delivery, gestational age at initiation and duration of the treatment, and indications of previous PTB were not different between the two groups. More women in the progesterone group who delivered at preterm received 200 mg than 100 mg progesterone and had shorter midtrimester cervical length than those who delivered at term. However, previous term birth history, number of previous PTB history, gestational age at delivery and indications of previous PTB were not significantly different between those who used 200 mg and 100 mg progesterone (data not shown). Multivariate analysis showed that midtrimester cervical length was significantly associated with the risk of recurrent PTB (OR, 0.920; 95% CI, 0.854-0.990; P=0.027), but dose of progesterone was not significantly associated with the risk of recurrent PTB (OR, 1.457; 95% CI, 0.385-5.520; P=0.580).
Discussion
In this retrospective study, we found that the rate of recurrent PTB in women with previous history of spontaneous PTB was over 40%, but the rate decreased to 21.9% when prophylactic vaginal micronized natural progesterone was used. The reduction of recurrent PTB after the treatment with vaginal micronized natural progesterone was statistically significant after controlling independent confounding factors. Our study is probably the first in Korea to report on progesterone treatment for prevention of PTB.
Early prediction and prevention is the most effective management of PTB. With the advances in obstetrics, a great advances were made in identification of risk factors for PTB, as well as early prediction of PTB such as measurement of cervical length and cervicovaginal fibronectin [21-24]. Risk factors of spontaneous PTB include prior history of PTB, ethnicity of pregnant women, multiple pregnancies, smoking, uterine anomaly and history of curettage or cervical conization [1,5]. Among these risk factors, prior PTB history is the most important factor and it can increase more than 2 fold of recurrence risk in their next pregnancy [7]. Defining risk factors and early prediction of PTB is important because it enables to recognize high-risk women and allows initiation of risk-specific treatment [5]. Progesterone is one of the few proven effective methods to prevent PTB in women with previous history of spontaneous PTB and in women with short cervical length [25].
The role and mechanism of progesterone in preventing PTB is not fully understood; it is known to relax the uterine smooth muscle, inhibition of oxytocin effects on the myometrium, and the formation of myometrial gap junction [10]. It has also been shown to regulate uterine contractility and prevent cervical ripening, which may play a role in onset of labor. Progestins are available in natural micronized or synthetic formulations for oral, intramuscular or vaginal administration. Also, the efficacy of progesterone for prevention of PTB varies depending on patient's characteristics, cervical length, history of PTB, and administration route or forms of progesterone.
Several studies reported 17α-hydroxyprogesterone caproate (17α-OHP-C) can prevent recurrent PTB in women with previous history of PTB [18,26]. However, there aren't any studies on the effect of 17α-OHP-C on prevention of PTB in women with short cervical length yet. Although there have been studies on gel type or oral vaginal micronized natural progesterone, there are still controversies on which subjects to be used [16,17,27,28]. In our study, we used micronized natural vaginal progesterone tablet in patients with PTB history because 17α-OHP-C and progesterone vaginal gel were not available in our hospital and we assumed that oral progesterone therapy might be ineffective for prevention of PTB.
Vaginal micronized natural progesterone was proved to be effective in preventing PTB in women with previous PTB history. In the randomized placebo-controlled trial of de Fonseca et al. [11], 100 mg of vaginal progesterone were used between 24 and 34 weeks of gestation in high risk women with history of previous PTB in over 90% of the subjects. They reported that progesterone was effective in preventing PTB (progesterone group 13.8% and non-user group 28.5%). Preterm birth before 34 weeks of gestation was significantly lower in progesterone group (2.8%) compared to placebo group (18.6%). In another randomized placebo-controlled trial of Majhi et al. [19], 100 mg of vaginal progesterone were used in women with previous PTB history from 20-24 to 36 weeks of gestation, and result showed that PTB rate was significantly lower in progesterone group than placebo group (12% vs. 38%; RR, 0.32; 95% CI, 0.14-0.72). In 2011, Cetingoz et al. [13], reported a randomized placebo controlled trial of 100 mg vaginal progesterone in high risk women starting from 24 to 34 weeks of gestation. The result showed that administering vaginal progesterone reduced preterm labor (25% vs. 45.7%, P<0.05), PTB before 37 weeks (40% vs. 57.2%, P<0.05) and 34 weeks (8.8% vs. 24.3%, P<0.05) of gestation. Our result also showed that vaginal micronized progesterone therapy was significantly associated with the reduction of PTB less than 37 weeks of gestation. However, the rate of recurrent PTB before 34 weeks of gestation decreased only from 20.3% to 17.8% with the use of vaginal progesterone and the difference was not statistically significant. This may be due to small number of study population and it is the main limitation of our study.
Short cervical length is one of the most important risk factor in PTB [21-24], and progesterone treatment is effective in reducing the risk of PTB in women with short cervical length [15,16]. Fetal Medicine Foundation reported a trial of approximately 24,000 low-risk women who were routinely checked for cervical length during their prenatal care [15]. 250 women with cervical length less than 15 mm were randomly allocated to receive 200 mg vaginal progesterone or placebo from 24 to 34 weeks of gestation. The result showed progesterone reduces the risk of spontaneous PTB before 34 weeks of gestation by 44.2% (19.2% vs. 34.4%; RR, 0.56; 95% CI, 0.36-0.86). In our study, we included women with previous PTB history, but 34.3% (56/163) of them had short cervical length less than 25 mm. Interestingly, although more women in the progesterone group had short cervical length, the risk of recurrent PTB was significantly lower in this group.
Dose of progesterone may be one of the important factors associated with preventing recurrent PTB. In previous studies, 100 mg progesterone was used in women with previous PTB history [11,13,19] and 200 mg progesterone was used in women with short cervical length [15]. But, in our study, there were no standardized criteria for the dose of progesterone and this is another main limitation of this retrospective study. We prescribed 100 mg progesterone to 30/73 (41.1%) women and 200 mg progesterone to 43/73 (58.9%) women. An intriguing result of our study was that more women in the progesterone group who delivered at preterm received 200 mg progesterone than those who delivered at term. This may be due to that more women who delivered at preterm had short cervical length than those who delivered at term. We tended to use 200 mg progesterone in women with short cervical length (25% vs. 45.7%, P<0.05). However, the result of our multivariate analysis showed that the dose of progesterone was not independently associated with risk of recurrent PTB.
Although this is the first report on the effect of progesterone therapy on preventing PTB in Korea, there still remain several limitations to our study. First, because of the retrospective nature of the study, the patients in both groups were heterogeneous in terms of patient selection, the dose of progesterone and the time of initiation and duration of the treatment. And information on compliance of medication and side effects of the vaginal progesterone were not available. Lastly, small number of patients is the main limitation to our study. Therefore, additional well-designed prospective studies are needed such as specific indications, optimal dose and regimen, optimal gestational age at initiation and end of treatment. In conclusion, micronized vaginal progesterone supplement therapy was associated with a significant reduction of recurrent PTB risk in women with previous spontaneous PTB history.



 XML Download
XML Download