

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Pyometra, a collection of purulent material in the uterus, is an uncommon gynecologic entity. Its reported incidence is 0.1% to 0.5% in gynecologic patients. However, the incidence increases to 13.6% in elderly women [1]. It usually develops in elderly women and may or may not be associated with malignancy. It is thought to be caused by occlusion of the cervical canal secondary to chronic cervicitis, radiation cervicitis, benign or malignant cervical lesions, puerperal infections, foreign bodies, or congenital anomalies. Also, the risk factors may include a decline in activity, incontinence, diabetes, and long-term intrauterine device use [2]. The classic triad of symptoms in patients with pyometra consists of purulent vaginal discharge, postmenopausal bleeding, and lower abdominal pain. However, more than 50% of all patients with nonruptured pyometra are asymptomatic [3]. Spontaneous perforation is a very rare complication of pyometra, but it must be considered in the differential diagnosis of peritonitis in elderly patients. Early diagnosis is very important in starting immediate treatment, thus reducing morbidity and mortality. Herein, we report a 78-year-old woman who was treated under a clinical diagnosis of diffuse peritonitis caused by spontaneously perforated pyometra and was confirmed as having cervical cancer, after surgery.
Case Report
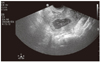
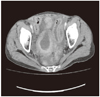
A 78-year-old multiparous woman who had no significant medical history visited our department of emergency medicine because of fever, vomiting, and diffused abdominal pain during the last 4 hours. Her gynecologic history was unremarkable without having undergone an eventful menopause. She had no history of postmenopausal bleeding or increased vaginal discharge. She had 6 pregnancies and all of her deliveries were normal vaginal. She had no history of sexually transmitted disease and claimed that she never had a Pap smear. She looked acutely ill with unstable vital signs (blood pressure 160/80 mm Hg, body temperature 37.8℃, and pulse rate 90 beats/min). Her abdomen was distended with rebound tenderness and varying tympanic sounds on percussion. Decreased bowel sounds and generalized tenderness of the lower abdomen were identified. Pelvic examination revealed an atrophic vulva and vagina. There was a small necrotic, sloughing, malignant-looking polyp extruding from the cervical os. The laboratory findings were as follows, white blood cell count 8,400/µL with 68.7% neutrophils, hemoglobin 11.3 g/dL, C-reactive protein 13.85 mg/dL, albumin 3.1 g/dL, glucose 205 mg/dL. Abdominal plain radiography disclosed an air-fluid level in the pelvic cavity, but subphrenic free air was not recognized. In transvaginal ultrasonography, the uterus felt bulky and an enlarged uterus with hypoechoic fluid collection was seen in the uterine cavity (Fig. 1). However, it was freely mobile, and the adnexa felt normal. Furthermore, both adnexa were not checked and in the cul-de-sac, a large amount of fluid collection was identified. Contrast-enhanced computed tomography (CT) showed multiple pelvic and intra-abdominal fluid collections, a dilated endometrial cavity with breach at the uterine fundus (Fig. 2).
She was diagnosed as having diffuse peritonitis due to a perforated pyometra and/or a gastrointestinal tract perforation, and thus exploratory laparotomy was performed. At the laparotomy, a large amount of purulent discharge arising from a perforated uterus was found in the abdominal cavity. The gastrointestinal tract and gallbladder had nonspecific findings. The fundus of the uterus was found to have a perforation, about 1.5 cm in diameter, with purulent discharge exuding from the lesion on compression (Fig. 3). The purulent discharge was aspirated and samples were sent for anaerobic and aerobic culture. A total hysterectomy with bilateral salpino-oophorectomy was performed. Macroscopically, it was showed cervical stenotic mass, dilated body and the necrotic endometrium. A histopathology of the resection specimen revealed pyometra with ischemic necrosis of the endometrium and invasive squamous cell carcinoma of the cervix with large cell keratinizing cervical cancer, which mainly involved the endocervix, measuring 1.3 cm in depth and 1.5 cm in length with free margins. The tumor marker of squamous cell carcinoma was also within normal limits; however, radiotherapy was arranged for the patient for a complete treatment of the disease. The surgical-pathologic staging was large cell keratinizing cervical squamous cell carcinoma stage Ib.
A bacteriological culture of the purulent fluid in the peritoneal cavity grew Escherichia coli (E. coli), but no anaerobic bacteria. Postoperatively, intensive antibiotics therapy was performed. Any respiratory and other complications, such as shock, disseminated intravascular coagulation or pneumonia, did not occur. She was discharged on the 12th postoperative day after managements.
Discussion
Spontaneously perforated pyometra is difficult to diagnose preoperatively. Its clinical findings usually mimic the symptoms of gastrointestinal tract diseases and a correct diagnosis can only be made by laparotomy. Missed diagnoses are common because of nonspecific symptoms and a rare condition. The most frequent preoperative diagnoses are generalized peritonitis, peumoperitoneum and perforated gastrointestinal tract, which lead to a misdiagnosis of gastrointestinal perforation [4]. However, a delayed diagnosis of perforated pyometra may lead to increased morbidity and mortality. CT features of perforated pyometra have been described in only 1 case in which CT suggested the diagnosis and surgical intervention was performed [5]. Ultrasound is a useful tool that has high sensitivity in assessing pyometra, but it plays a limited role in the diagnosis of perforated pyometra because of its inability to demonstrate the uterine breach and the limited sonographic window available due to perforation. Preoperative cervical cytology is important in ruling out cervical diseases. In our case, the patient presented with features of generalized peritonitis, and CT scan showed perforated pyometra at the uterine fundus with multiple pelvic and intra-abdominal fluid collections.
A spontaneous perforation of pyometra and subsequent diffuse peritonitis are rare, with the incidence being about 0.01%-0.05%. Benign or malignant conditions cause accumulation of secretion and gradual enlargement of the uterus, occur at the site of degenerative or necrotic change and lead to thinned uterine walls which may be sloughed with spontaneous perforation and causing generalized peritonitis. Imachi et al. [6] reviewed 14 cases of spontaneous perforation of pyometra and stated that only 5 cases were associated with malignant diseases, consisting of 2 cervical cancers, 2 colon cancers, and 1 endometrial cancer. Spontaneous uterine perforation is rare. An extensive review of the English literature has revealed only 26 such reported cases to date. Furthermore, spontaneous rupture of pyometra in cervical cancer presenting as generalized peritonitis is extremely rare and only 4 cases have been reported [7]. The most common presenting symptoms and sign are abdominal pain, vomiting, nausea, fever and enlargement of the uterus [8]. The most common perforation site is the uterine fundus. Leukocytosis may not occur in elderly patients with perforated pyometra, even though generalized peritonitis occurs, as in our patient [9].
The treatment methods for pyometra include proper drainage of the uterine cavity and administration of antibiotics effective against aerobic and anaerobic bacteria. The most common etiological organisms is E. coli which is facultatively anaerobic [10]. Since perforated pyometra is difficult to diagnose preoperatively, it requires emergency operation. Hysterectomy with bilateral salpingo-oophorectomy may be the best choice for perforated pyometra, because peritoneal lavage with drainage is not effective in the control of infection [11]. However, because such patients are elderly, under poor general conditions, and often with unfavorable prognoses, intensive pre- and postoperative care of respiratory and circulation is essential [12]. Cases of spontaneously perforated pyometra associated with non-malignancy have better prognoses than those with malignancy. Saha et al. [13] reported that 73% of the non-malignancy cases had favorable prognoses for survival, whereas only 33% of malignancy cases did.
In conclusion, a diagnosis of spontaneous perforation of pyometra is rarely made preoperatively, and thus the possibility of perforated pyometra should be considered when elderly women suffer from acute abdominal pain. We reported a patient who was admitted due to spontaneously perforated pyometra, was successfully treated with total abdominal hysterectomy and bilateral salpingo-oophorectomy and she discharged without complications.

 XML Download
XML Download