

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Dilatation and curettage (D&C) is one of the most frequently performed procedures for first trimester surgical abortion, also nonobstetric D&C can be performed for both diagnostic and therapeutic indications. The mortality and morbidity of D&C are very low, and perforation of uterus is rare. But curettage of a large, soft postpartum uterus can be a formidable undertaking because the risk of perforation is high and the procedure commonly results in increased rather than decreased bleeding. Although many perforations are innocuous, others lead to infection, hemorrhage, and trauma to abdominal contents. Bowel perforation is an infrequent complication, it persists as an important cause of peritonitis and sepsis. The following cases describe two women, who suffered intestinal perforation after D&C at delayed postpartum period.
Figures and Tables
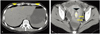
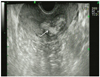
Fig. 1
(A) Precontrast abdomen and pelvis computed tomography shows multiple peritoneal free gas (arrow head) and ascites (arrow). (B) Enlarged uterus with 33 × 21 mm sized intestine like enhancing mass in uterine cavity was shown (arrow head) in contrast inhanced abdomen and pelvis computed tomography.
References
1. Strauss LT, Herndon J, Chang J, Parker WY, Levy DA, Bowens SB, et al. Abortion surveillance: United States, 2001. MMWR Surveill Summ. 2004. 53:1–32.
2. Poggi S, Kapernick P. DeCherney AH, Nathan L, editors. Postpartum hemorrhage & the abnormal puerperium. Current obstetrics & gynecologic diagnosis & treatment. 2007. 10th ed. New York: McGraw-Hill;1559–1579.
3. Grimes DA, Schulz KF, Cates WJ Jr. Prevention of uterine perforation during curettage abortion. JAMA. 1984. 251:2108–2111.
4. Hefler L, Lemach A, Seebacher V, Polterauer S, Tempfer C, Reinthaller A. The intraoperative complication rate of nonobstetric dilation and curettage. Obstet Gynecol. 2009. 113:1268–1271.
5. Hakim-Elahi E, Tovell HM, Burnhill MS. Complications of first-trimester abortion: a report of 170,000 cases. Obstet Gynecol. 1990. 76:129–135.
6. Lassey AT. Complications of induced abortions and their preventions in Ghana. East Afr Med J. 1995. 72:774–777.
7. Shulman SG, Bell CL, Hampf FE. Uterine perforation and small bowel incarceration: sonographic and surgical findings. Emerg Radiol. 2006. 13:43–45.
8. Cunningham FG, Leveno KJ, Bloom SL, Hauth JC, Rouse DJ, Spong CY. Cunningham F, Leveno K, Bloom S, Hauth J, Rouse D, Spong C, editors. Abortion. Williams obstetrics. 2010. 23rd ed. New York: McGraw-Hill;215–234.
9. Imoedemhe DA, Ezimokhai M, Okpere EE, Aboh IF. Intestinal injuries following induced abortion. Int J Gynaecol Obstet. 1984. 22:303–306.
10. Kambiss SM, Hibbert ML, Macedonia C, Potter ME. Uterine perforation resulting in bowel infarction: sharp traumatic bowel and mesenteric injury at the time of pregnancy termination. Mil Med. 2000. 165:81–82.
11. Coffman S. Bowel injury as a complication of induced abortion: a case report and literature review. Am Surg. 2001. 67:924–926.
12. Tavakkolizadeh A, Whang EE, Ashley SW, Zinner MJ. Brunicardi FC, Andersen DK, Billiar TR, Dunn DL, Hunter JG, Matthews JB, editors. Small intestine. Schwartz's principles of surgery. 2010. 9th ed. New York: McGraw-Hill;120–135.
13. Hoveyda F, MacKenzie IZ. Secondary postpartum haemorrhage: incidence, morbidity and current management. BJOG. 2001. 108:927–930.
 XML Download
XML Download