

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Radical trachelectomy was proposed to preserve fertility in women with early stage cervical cancer [1,2]. However, it is clear that cervical incompetence (CI), which leads to very early preterm birth, is common in pregnancy following radical trachelectomy [3,4]. We report a successful term pregnancy after transabdominal cerclage (TAC) with previous second trimester loss following vaginal radical trachelectomy (VRT).
Case Report
A 29-year-old nulliparous woman presented to our institution for evaluation of a high-grade squamous intraepithelial lesion identified on her Pap smear. A cervical punch biopsy showed a cervical intraepithelial neoplasia (CIN) III, and the patient underwent conization. The histology showed invasive squamous cell carcinoma with more than 4 mm in depth. She was assessed by clinical evaluation and was staged International Federation of Obstetrics and Gynecology (FIGO) stage IB1.
As she strongly desired to preserve her fertility, she underwent VRT with laparoscopic bilateral lymphadenectomy. She was informed of the possibility of preterm birth after VRT. A concurrent prophylactic cerclage using monofilament nonabsorbable polyprophylene (1-0 Prolene, Ethicon, Somerville, NJ, USA) was performed. The histology demonstrated invasive squamous cell carcinoma with 5 mm in depth and no involvement of resection margins. No lymphatic or vascular invasion was observed on pathology.
A year later, she conceived spontaneously. However, she lost the fetus at 20 weeks of gestation resulting from CI. Next year, she presented to our institution for her second spontaneous pregnancy. She was in good health and her repeat Pap smear showed negative intraepithelial lesion.
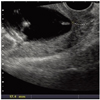
Transvaginal ultrasonography revealed short cervical length of "neo-cervix" (17.4 mm) with no funneling (Fig. 1). An additional cerclage was essential for preventing CI in her second pregnancy.
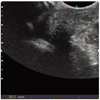
As no residual cervical tissue was remained suitable for additional vaginal cerclage, TAC using Mersilene tape was performed at 13 2/7 weeks of gestation. There was no intraabdominal adhesion at the time of TAC. Postoperatively, transvaginal ultrasonography (TVU) revealed a cervical length of 23.7 mm with no funneling (Fig. 2). She was discharged home without any postoperative complication, and was not restricted with movement. Her cervical length remained 20 mm at 35 weeks of gestation (Fig. 3). She showed no symptom or sign of preterm labor or preterm premature rupture of membrane (PPROM) or chorioamnionitis throughout the pregnancy.
At 39 6/7 weeks of gestation, she delivered healthy living female weighing 2,940 g via elective Cesarean section. We untied TAC knot because she did not desire to conceive anymore. Both mother and neonate were discharged well. Her postpartal Pap smear demonstrated negative lesion. She still thrives without any evidence of recurrence of cervical cancer.
Discussion
The optimal goal of pregnancy following radical trachelectomy is to deliver a viable infant. The lack of mechanical support and mucus of normal cervix could lead to CI and ascending infection [3,5]. The risk of second-trimester loss (9%-.10%) is much higher than general population (approximately 3%) in radical trachelectomy group [1]. Cerclage placement is the only option to preclude CI. However, it is difficult to place vaginal cerclage in the "neo-cervix" following radical trachelectomy. Although permanent prophylactic cerclage was performed at the time of VRT, our patient lost her first baby resulting from CI. Therefore, we elected transabdominal approach to place additional protective cerclage. The prolongation after TAC was 186 days. She did not demonstrate any symptoms or signs of preterm labor or PPROM, which is common in pregnancy following radical trachelectomy. Finally she succeeded in her second pregnancy without complication.
A woman undergoing VRT does not have enough cervical tissue for supplementary vaginal cerclage, because cervix is amputated below cervical isthmus at the time of VRT. As TAC knot is placed higher than transvagincal cerclage, a slippage of the knot and an ascending infection may be decreased [6,7]. We suppose TAC could prevent CI and ascending infection following radical trachelectomy. Although we performed TAC following VRT, we presume that preconceptional TAC at the time of radical trachelectomy might improve pregnancy outcome. TVU follow-up is prudent after TAC for the evaluation of cervical competence. Excessive pressure by the TVU examiner should be avoided as the cervix has markedly modified anatomy after VRT. We conclude that TAC is an acceptable option to preclude CI in pregnant women following radical trachelectomy and the combination of postoperative TVU and other adjunctive strategies could reduce the rate of preterm birth after radical trachelectomy.

 XML Download
XML Download