

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The condition termed 46,XY complete gonadal dysgenesis, also known as 'Swyer's syndrome', is characterized by the lack of testicular determination with resulting streak gonads, normal Mullerian structures, and female external genitalia. Because of incomplete testicular determination in the patient with 46,XY partial gonadal dysgenesis, mullerian structures may be present or absent, and the external genitalia may be female, ambiguous, or male [1]. The increased potential for gonadal malignancy in patients with XY gonadal dysgenesis is well-documented [2]. Therefore, prophylactic gonadectomy is indicated soon after diagnosis.
In Swyer's syndrome, because the streak gonads are located in the normal adnexal location adjacent to the uterus, a laparoscopic gonadectomy can be easily performed by experienced gynecologists [3-5]. However, if streak gonads are located in unusual sites, especially in inguinal canals, it is not easy to identify the streak gonads because the gonads are thin and small.
We present our experience with the laparoscopic removal of streak gonads within the inguinal canals in a patient with XY partial gonadal dysgenesis.
Case Report
A 33-year-old woman (height, 168 cm; weight, 60 kg) presented with primary amenorrhea. The physical examination revealed no breast development (Tanner stage I), scanty axillary and pubic hair (Tanner stage II), and normal female external genitalia. The gynecologic examination revealed a short blind vaginal pouch (approximately 3 cm in depth) with no palpable uterus or cervix. There were no palpable gonads in the inguinal area or labium majora bilaterally.
Laboratory tests revealed an elevated follicle stimulating hormone (60.3 mIU/mL) and luteinizing hormone (34.5 mIU/mL), and a decreased estradiol (<5 pg/mL). The total testosterone level (0.80 ng/mL) was at the upper limit of normal for females. Chromosomal analysis showed a normal male karyotype (46, XY). Neither a uterus nor gonads were noted on transvaginal ultrasound and magnetic resonance imaging (MRI) scans.
Based on a diagnosis of XY gonadal dysgenesis, we planned a prophylactic laparoscopic gonadectomy due to the malignant potential of streak gonads.
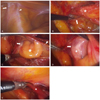
Under general anesthesia the patient was placed in the low lithotomy position. A primary trocar was inserted in the umbilicus, 2 ancillary trocars were placed in the left side of the abdomen, and 1 ancillary trocar was placed in the right side of the abdomen. The laparoscopic findings revealed that there was no uterus or no visible gonads in the abdomen and pelvic cavity. Bilateral gonadal vessels were identified lateral to the external iliac arteries and the distal ends of the vessels entered the internal inguinal rings (Fig. 1A). A peritoneal incision was made along the gonadal vessel, and further dissection in the direction of the inguinal area revealed a spermatic cord and the internal inguinal ring (Fig. 1B). Because the streak gonad was located within the spermatic cord, we could not identify the distal end of the gonad. Therefore, the spermatic cord was opened with monopolar scissors. The streak gonad was a white band-like structure and the epididymis was within the spermatic cord (Fig. 1C). After identifying the distal end of the streak gonad (Fig. 1D), the vas deferens (distal to the gonad) was transected with LigaSure (10 mm laparoscopic instrument; Valleylab [a branch of Covidien], Boulder, CO, USA) (Fig. 1E). The contralateral streak gonad and epididymis were excised using the same method. A prophylactic herniorrhaphy using polyprophylene mesh was performed due to weakening of the internal inguinal ring from dissection. Reperitonealization was performed using laparoscopic suturing.
The pathologic findings of the gonads showed that dysgenetic testes, without evidence of malignancy, consisted of immature Sertoli cells without spermatogenesis and immature Leydig cells. Immature epididymis and vas deferens tissues were also founded. The diagnosis of XY partial gonadal dysgenesis was established.
The postoperative course was uneventful, and the patient was discharged from the hospital after 48 hours. The patient has been prescribed estrogen replacement therapy.
Discussion
In patient with 46,XY partial gonadal dysgenesis, mullerian structures may be present or absent, and the external genitalia may be female, ambiguous, or male. Due to variable internal and external genitalia, the diagnosis of XY partial gonadal dysgenesis might be difficult. The difference between 46,XY partial gonadal dysgenesis and XY complete gonadal dysgenesis (Swyer's syndrome) is that the uterus and fallopian tubes may be absent in the partial form. In the case presented herein, the findings of external female genitalia with a blind vaginal pouch, internal male genitalia, and gonads within the inguinal canals were consistent with androgen insensitivity syndrome. However, in patients with androgen insensitivity syndrome, secondary sexual characteristics are present and the gonads are testes. Patients with mixed gonadal dysgenesis have asymmetric gonadal dysgenesis in which one gonad is a testis and the other gonad is a streak gonad or absent. Therefore, mixed gonadal dysgenesis was not the diagnosis in the current case based on the pathologic findings.
Previously, prophylactic gonadectomy was performed by laparotomy in phenotypic females with a Y choromsome. In 1990, the first laparoscopic adnexectomy was performed in a 12-year-old patient with pure gonadal dysgenesis [4]. In 1991, the first laparoscopic bilateral gonadectomy was reported in a patient with androgen insensitivity syndrome [6]. In patients with androgen insensitivity syndrome, a laparoscopic gonadectomy is generally not difficult, even if the testes are present within the inguinal canals [7]. Simultaneous external digital compression on the gonads located in the inguinal canals and intra-abdominal traction with grasping forceps allows the gonads to be replaced into the abdominal cavity [8]. In addition, the testes in patients with androgen insensitivity syndrome are generally normal gonadal size and can be easily identified.
However, if streak gonads are present in the inguinal canals, the exact location of the gonads cannot be easily identified by physical examination, ultrasonography, MRI, and laparoscopic finding, as shown in the current case. During prophylactic gonadectomy, to identify and excise whole streak gonads is mandatory because remnant gonads have a risk of malignancy. As shown in this report, opening of the spermatic cord will be of help to identify streak gonads. As long as the distal margin of the streak gonad is identified, excision of the vas deferens distal to the gonad is not difficult.
Identifying dysgenetic gonads is not always easy [9]. When gonads cannot be found in the abdominopelvic cavity, after peritoneal incision along the gonadal vessels, dissection in the direction of the inguinal canal is of help to find dysgenetic gonads.
When the dysgenetic gonads are located deep within the inguinal canals, requiring extensive dissection of the inguinal ring may result in the subsequent risk of an inguinal hernia [8]. However, the true incidence of hernia in such cases has not been known. Although the necessity of prophylactic herniorrhaphy is uncertain, we believe that prophylactic herniorrhaphy to prevent inguinal hernias will be beneficial when the inguinal canal is weakened due to aggressive dissection of the inguinal canal.
A laparoscopic approach for prophylactic gonadectomy in patients with XY gonadal dysgenesis is feasible, even if streak gonads are present within the inguinal canals.
 XML Download
XML Download