

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Vesicovaginal fistulas are a most common complication accompanied by gynecologic surgeries, but other types of fistulas rarely occur. Especially rectovesical fistulas arising post-operative complication occur in extremely lower possibility and very few cases have been reported in the world. Interestingly, our case showed a symptom of urinary drainage from the anus unlike other cases with pneumaturia or fecaluria. This symptom could hardly happen because urine is prevented from being released due to the internal pressure of the fistula. We experienced and treated a first case of rectovesical fistula with a symptom of passing urine from the anus.
Figures and Tables
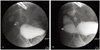
Fig. 1
Cystography shows drainage of contrast medium in the bladder (arrow) into the proximal rectum (open arrow). (A) Immediately after injection of contrast medium into the bladder. (B) Two minutes after injection.

References
1. Forsgren C, Altman D. Risk of pelvic organ fistula in patients undergoing hysterectomy. Curr Opin Obstet Gynecol. 2010. 22:404–407.
2. Han CH, Lee YS, Kang SH, Lee JW, Park TC. Clinical characteristics of urinary-vaginal fistulas after various types of hysterectomy. Korean J Obstet Gynecol. 2005. 48:2205–2210.
3. El-Tabey NA, Ali-El-Dein B, Shaaban AA, El-Kappany HA, Mokhtar AA, El-Azab M, et al. Urological trauma after gynecological and obstetric surgeries. Scand J Urol Nephrol. 2006. 40:225–231.
4. Hawary A, Clarke L, Taylor A, Duffy P. Enterovesical fistula: a rare complication of urethral catheterization. Adv Urol. 2009. 591204.
5. Scozzari G, Arezzo A, Morino M. Enterovesical fistulas: diagnosis and management. Tech Coloproctol. 2010. 14:293–300.
6. Altman D, Forsgren C, Hjern F, Lundholm C, Cnattingius S, Johansson AL. Influence of hysterectomy on fistula formation in women with diverticulitis. Br J Surg. 2010. 97:251–257.
7. Garcea G, Majid I, Sutton CD, Pattenden CJ, Thomas WM. Diagnosis and management of colovesical fistulae; six-year experience of 90 consecutive cases. Colorectal Dis. 2006. 8:347–352.
8. Kavanagh D, Neary P, Dodd JD, Sheahan KM, O'Donoghue D, Hyland JM. Diagnosis and treatment of enterovesical fistulae. Colorectal Dis. 2005. 7:286–291.
9. Narayanan P, Nobbenhuis M, Reynolds KM, Sahdev A, Reznek RH, Rockall AG. Fistulas in malignant gynecologic disease: etiology, imaging, and management. Radiographics. 2009. 29:1073–1083.
10. Dawam D, Patel S, Kouriefs C, Masood S, Khan O, Sheriff MK. A "urological" enterovesical fistula. J Urol. 2004. 172:943–944.
11. Murakami K, Tomita M, Kawamura N, Hasegawa M, Nabeshima K, Hiki Y, et al. Severe metabolic acidosis and hypokalemia in a patient with enterovesical fistula. Clin Exp Nephrol. 2007. 11:225–229.
12. Thomas K, Williams G. Medicolegal aspects of vesicovaginal fistulae. BJU Int. 2000. 86:354–359.
13. Duong TH, Gellasch TL, Adam RA. Risk factors for the development of vesicovaginal fistula after incidental cystotomy at the time of a benign hysterectomy. Am J Obstet Gynecol. 2009. 201:512.e1–512.e4.
14. Ng CC, Chern BS, Siow AY. Retrospective study of the success rates and complications associated with total laparoscopic hysterectomy. J Obstet Gynaecol Res. 2007. 33:512–518.
15. Kim BY, Yang JB, Lee MA, Ko YB, Lee KH. Laparoscopic repair of vesicovaginal fistula. Korean J Obstet Gynecol. 2009. 52:278–284.
 XML Download
XML Download