

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Objective
To compare the clinical characteristics, hematologic findings, microbiologic results of Fitz-Hugh-Curtis syndrome (FHCS) to uncomplicated pelvic inflammatory disease (PID).
Methods
We retrospectively reviewed the medical records of 41 patients of FHCS and 52 patients of uncomplicated PID in Myongji Hospital from January 2007 to August 2011. Between the two groups, we compared clinical manifestations, physical examination findings, hematologic findings, microbiologic study findings, abdomen and pelvic computed tomography.
Results
FHCS accounted for 14.3% of total cases of pelvic inflammatory disease at our medical institution. Patients of both groups visited with a chief complaint of abdominal pain. The most common symptom was the right upper quadrant (RUQ) pain (78.0%) in the FHCS group and the pelvic pain (75%) in the uncomplicated PID group. The incidence of pelvic organ tenderness and cervical motion tenderness was lower in the FHCS group as compared with the uncomplicated PID group. FHCS group was associated with significantly higher C-reactive protein level in comparison to that of uncomplicated PID group (P = 0.0175). In addition, higher incidence of chlamydial infection was noted in FHCS group.
Figures and Tables
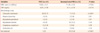
 | Fig. 1Arterial phase of abdomino-pelvic contrast-enhanced computed tomography of a 37-year-old woman who complaint right upper quadrant abdominal pain. Hepatic capsular enhancement is seen at the surface of the medial segment and the lateral aspect of the right lobe.
|
Table 1
General characteristics of the patients
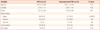
Values are presented as mean ± standard deviation (SD) or number (%).
Statistical analysis of age, parity, gravida was done with t-test. And analysis of remainders was done with chi-square test.
FHCS, Fitz-Hugh-Curtis syndrome; PID, pelvic inflammatory disease; NA, not assessed; IUD, intra-uterine device.
![]()
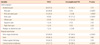
Table 3
laboratory findings
Values are presented as mean±standard deviation or number (%), permit duplicated count in co-infected cases.
Statistical analysis of WBC count, CRP was done with t-test. And analysis of microbiologic tests was done with chi-square test.
FHCS, Fitz-Hugh-Curtis syndrome; PID, pelvic inflammatory disease; WBC, white blood cell; CRP, C-reactive protein.
![]()
References
1. Curtis AH. A cause of adhesions in the right upper quadrant. JAMA. 1930. 94:1221–1222.
2. Fitz-Hugh T Jr. Acute gonococcic peritonitis of the right upper quadrant in women. JAMA. 1934. 102:2094–2096.
3. Stajano C. La reaccion frenica en ginecologica. Sem Med. 1920. 27:243–248.
4. Curtis AH. Adhesions of the anterior surface of the liver. JAMA. 1932. 99:2010–2012.
5. Wang SP, Eschenbach DA, Holmes KK, Wager G, Grayston JT. Chlamydia trachomatis infection in Fitz-Hugh-Curtis syndrome. Am J Obstet Gynecol. 1980. 138:1034–1038.
6. Semchyshyn S. Fitz-Hugh and Curtis syndrome. J Reprod Med. 1979. 22:45–48.
7. Onsrud M. Perihepatitis in pelvic inflammatory disease: association with intrauterine contraception. Acta Obstet Gynecol Scand. 1980. 59:69–71.
8. Müller-Schoop JW, Wang SP, Munzinger J, Schläpfe HU, Knoblauch M, Tammann RW. Chlamydia trachomatis as possible cause of peritonitis and perihepatitis in young women. Br Med J. 1978. 1:1022–1024.
9. Dalaker K, Gjonnaess H, Kvile G, Urnes A, Anestad G, Bergan T. Chlamydia trachomatis as a cause of acute perihepatitis associated with pelvic inflammatory disease. Br J Vener Dis. 1981. 57:41–43.
10. Wølner-Hanssen P, Svensson L, Weström L, Mårdh PA. Isolation of Chlamydia trachomatis from the liver capsule in Fitz-Hugh-Curtis syndrome. N Engl J Med. 1982. 306:113.
11. Lopez-Zeno JA, Keith LG, Berger GS. The Fitz-Hugh-Curtis syndrome revisited. Changing perspectives after half a century. J Reprod Med. 1985. 30:567–582.
12. Vickers FN, Maloney PJ. Gonococcal perihepatitis. Report of three cases with comments on diagnosis and treatment. Arch Intern Med. 1964. 114:120–123.
13. Banerjee B, Rennison A, Boyes BE. Sonographic features in a case of Fitz-Hugh-Curtis syndrome masquerading as malignancy. Br J Radiol. 1992. 65:342–344.
14. Money DM, Hawes SE, Eschenbach DA, Peeling RW, Brunham R, Wölner-Hanssen P, et al. Antibodies to the chlamydial 60 kd heat-shock protein are associated with laparoscopically confirmed perihepatitis. Am J Obstet Gynecol. 1997. 176:870–877.
15. Wølner-Hanssen P. Oral contraceptive use modifies the manifestations of pelvic inflammatory disease. Br J Obstet Gynaecol. 1986. 93:619–624.
16. Litt IF, Cohen MI. Perihepatitis associated with salpingitis in adolescents. JAMA. 1978. 240:1253–1254.
17. Jacobson L, Westrom L. Objectivized diagnosis of acute pelvic inflammatory disease. Diagnostic and prognostic value of routine laparoscopy. Am J Obstet Gynecol. 1969. 105:1088–1098.
18. Holschneider CH, Berek JS. Berek JS, Novak E, editors. Genotiurinary infections and sexually transmitted disease. Berek & Novak's gynecology. 2007. 14th ed. Philadelphia (PA): Lippincott Williams & Wilkins;549–551.
19. Nishie A, Yoshimitsu K, Irie H, Yoshitake T, Aibe H, Tajima T, et al. Fitz-Hugh-Curtis syndrome. Radiologic manifestation. J Comput Assist Tomogr. 2003. 27:786–791.
20. Tsubuku M, Hayashi S, Terahara A, Furukawa T, Ohmura G. Fitz-Hugh-Curtis syndrome: linear contrast enhancement of the surface of the liver on CT. J Comput Assist Tomogr. 2002. 26:456–458.
21. Ris HW. Perihepatitis (Fitz-Hugh--Curtis syndrome). A review and case presentation. J Adolesc Health Care. 1984. 5:272–276.
22. McCormack WM. Pelvic inflammatory disease. N Engl J Med. 1994. 330:115–119.
23. Miettinen AK, Heinonen PK, Laippala P, Paavonen J. Test performance of erythrocyte sedimentation rate and C-reactive protein in assessing the severity of acute pelvic inflammatory disease. Am J Obstet Gynecol. 1993. 169:1143–1149.
24. Peter NG, Clark LR, Jaeger JR. Fitz-Hugh-Curtis syndrome: a diagnosis to consider in women with right upper quadrant pain. Cleve Clin J Med. 2004. 71:233–239.
25. Clinical Effectiveness Group (Association of Genitourinary Medicine and the Medical Society for the Study of Venereal Diseases). National guideline for the management of pelvic infection and perihepatitis. Sex Transm Infect. 1999. 75:Suppl 1. S54–S56.
26. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines 2002. MMWR Recomm Rep. 2002. 51:1–78.
27. Stamm WE. Kasper DL, Braumwald E, Fauci AS, Hauser SL, Longo DL, Jamesn JL, editors. Chlamydial infections. Harrison's principles of internal medicine. 2005. 16th ed. New York (NY): McGrow-hill;1016.
 XML Download
XML Download