

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Acute abdominal pain is one of the most common presenting symptoms of emergency department patients. The classic guidelines in surgical medicine are that abdominal pain with diarrhea suggests a diagnosis of gastroenteritis [1]. However, a substantial number of these patients need emergency surgical intervention. In one retrospective study which evaluated emergency patients with abdominal pain and diarrhea, 9% of such patients underwent emergency surgery [2]. Of note, torsion of a pedunculated subserosal uterine leiomyoma can also present with acute abdominal pain and diarrhea.
A literature search on this topic does not yield many specific reports of leiomyoma-related complications or the presenting features [3]. Herein, we describe one case of torsion of a pedunculated subserosal uterine leiomyoma in a woman who noticed lower abdominal pain with severe diarrhea, which was assumed to be typical acute gastroenteritis.
Case Report
A 25-year-old virgin sought evaluation in our emergency department with acute lower abdominal pain and diarrhea on 21 January 2010. The abdominal pain developed 2 days ago, and increased in intensity over the past few hours. She had 10 episodes of watery diarrhea per day. Prior to presenting to our emergency room, she received conservative treatment at a local clinic for presumptive acute gastroenteritis; however, the symptoms did not improve, even though she was taking probiotics and analgesics. Contrast-enhanced abdominal computerized tomography scan revealed a non-enhanced pelvic mass connected to the posterior aspect of the uterine corpus with a distinct border, measuring 6.7 × 5.9 × 6.3 cm, with a small amount of ascites. Others including both ovaries were unremarkable (Fig. 1). She was referred to our emergency department. On physical examination, the temperature was 37.8℃, and there was direct and rebound tenderness in the left lower abdomen. The white blood cell count was 11,430/µL (normal value 4,000-10,000/µL) with 80.1% segment neutrophils (normal value 40.0-74.0%), and C-reactive protein was elevated to 5.7 mg/dL (normal value < 0.3 mg/dL). The stool specimen was negative for white blood cells and hemoglobin, and the Widal test was negative. Plain abdominal X-ray showed a mild ileus bowel gas pattern after computerized tomography scan (Fig. 2). A transrectal ultrasound showed a deviated uterus with a heterogenous echoic globular mass, measuring 6.1 × 5.6 × 5.4 cm in the culde-sac, with a small amount of fl uid (Fig. 3). We suspected that it could be torsion or infection of a pedunculated subserosal uterine leiomyoma.
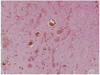
The patient underwent an emergency diagnostic laparoscopy under general anesthesia on the day of admission. At the time of laparoscopy, a dark blue subserosal leiomyoma, approximately 6 cm in size, was identified on a twisted pedicle to the posterior surface of the uterus. Hemorrhagic changes in the leiomyoma and hyperemic changes in the bowel serosa were noted. The bilateral fallopian tubes and ovaries were grossly normal and there was approximately 50 mL of ascites. An uncomplicated laparoscopic myomectomy was performed. On histopathologic report, leiomyomatous tissue with multifocal hemorrhage and congestion was noted with dilatated vessels (Fig. 4). The diarrhea stopped and the post-operative course was uneventful. She was discharged from the hospital on 4th operation day.
Discussion
Acute onset of abdominal pain is an unusual presenting complaint for uterine leiomyoma. The pain is usually related to complications involving a subserosal leiomyoma, including red degeneration, torsion, mesenteric vein thrombosis, and intestinal gangrene [4]. Contrary to expectations, a literature search on torsion of uterine subserosal leiomyoma yields just six cases all over the world and this report is the second in Korea. Torsion is a rare complication and most of patients are asymptomatic or complain nonspecific abdominal pain; therefore, preoperative diagnosis is very difficult [5,6]. Because an early diagnosis and surgical exploration are crucial to avoid life-threatening conditions like consumptive coagulopathy by ischemic gangrene and peritonitis, if suspected, diagnosis and treatment by laparoscopy should be considered [4,5]. In the current case, the patient presented with constant lower abdominal pain and watery diarrhea. The variability of symptoms and clinical features of serious causes of abdominal pain have increased the need for diagnostic imaging during the evaluation of these patients.
Transvaginal ultrasound may identify a lesion lateral to the uterus, and color Doppler on the twisted pedicle could imply torsion of a leiomyoma in some cases. Finding an abrupt cutoff or even twisting of the pedicle on color Doppler may suggest the diagnosis, but those patterns are not regularly depicted [6]. Doppler ultrasound can demonstrate normal adnexal and uterine arterial waveforms, but these do not exclude torsion [6]. The ultrasound of this patient showed a solid uterine mass with heterogenous echogenicity, which may mean the beginning of necrotic degeneration [7]. Regrettably, color Doppler ultrasound could not be performed due to emergency department equipment settings at that time. However, the findings on abdominal computerized tomography scan clarified the anatomic relationship and led to accurate diagnosis. Roy et al. [6] proposed a diagnosis of acute torsion of subserosal leiomyomas when normal ovaries and contrast enhancement of the uterine portion connected to the mass are present on abdominal computerized tomography scan. An abdominal computerized tomography scan of this patient was obtained 1 day after onset; the entire lesion showed no enhancement, which indicates complete interruption of blood fl ow and infarction [8]. The continuity of the mass with the uterus indicated that the origin of the mass was the uterine corpus. Together, the moderately contrast-enhanced uterine corpus with a non-enhanced mass suggested torsion of a pedunculated subserosal uterine leiomyoma.
In this case, obstruction of the arterial supply produced hemorrhagic change and congestion with dilated vessels, which are typical pathologic features of torsion. Two days after acute torsion, hemorrhagic infarction of the involved leiomyoma may be followed by necrosis, then peritonitis [8]. These changes could cause acute severe diarrhea, which resolved following surgical removal by emergency laparoscopy. We presented a patient with acute torsion of a pedunculated subserosal uterine leiomyoma causing abdominal pain and severe diarrhea. If women with acute diarrhea do not improve by empirical treatment, a surgical abdomen such as acute torsion of a subserosal leiomyoma should be considered. To facilitate prompt diagnosis and management, imaging techniques like ultrasound and an abdominal computerized tomography scan are essential. Once the diagnosis is made or suspected, surgical exploration is indicated and excision of the lesion can be sufficient.



 XML Download
XML Download