

 PDF
PDF ePub
ePub Citation
Citation Print
Print



The occurrence of ectopic decidua (deciduosis) has been observed most often in the cervix and appendix [1]. It has been established in approximately 90% of patients who have undergone laparotomy during pregnancy [2]. Ovarian deciduosis, however, is a less frequent in pregnancy. Ectopics decidua is a physiological phenomenon of pregnancy and arises from a progesterone-induced metaplasia of subserosal stromal cells [2,3]. We experienced an unusual case of ovarian deciduosis found at 21 weeks gestation in a primigravida with features of ovarian cyst.
Case Report
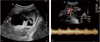
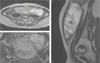
A 32-year-old woman, gravida 1, para 0, abortus 0 was referred to our institute because of an accidentally detected left ovarian cyst at 21 weeks gestation. She had no significant medical or gynecological history before. On admission, transvaginal ultrasound scan showed 10.9 × 3.9 cm sized heterogenous cystic mass with solid portion. The peritoneal cavity was filled with small amount of free fluid. Doppler utrasonogram image of the mass shows vascularization with pulsatility, a finding that is suggestive of a malignant mass (Fig. 1) [4,5]. The magnetic resonance imaging also showed 10 × 7 × 4.8 cm sized mass lesion consisted of multicystic component and large amount of solid component, mainly along the cyst wall suggestive of left ovarian tumor, borderline to malignancy (Fig. 2) [4,5].
As the result of the imaging studies was suspicious for malignancy, we thoroughly explained the natural history, prognosis of disease, available treatment methods, and their possible risks and discussed with the patient and her family. At last, they decided to conserve pregnancy. An exploratory laparotomy was planned at 21 weeks gestation. Through a midline incision, laparotomy was performed in the supine position. Intraoperative findings revealed about 12 × 6 × 8 cm sized multiloculated mass on the left ovary, with mixed serous and solid portion. The tubes and uterus were grossly normal. The left salpingo-oophorectomy was done. A piece of ovarian tissue was taken for histopathological examination. Frozen sections of the mass revealed a benign cyst that might be a mucinous cystadenoma. The surgery has been completed successfully. Postoperatively patient was treated with antibiotics and tocolytics. After uneventful recovery she was discharged on 11st postoperative day with ongoing pregnancy. The rest of the pregnancy was unremarkable. At 40 weeks gestation an uneventful vaginal delivery resulted in a 3,440 g normal male baby with Apgar of 7/10 and 8/10. She was doing well at the 6 month follow-up after delivery.
1. Pathological findings
On microscopic examination, nest of epithelioid cells in small islands were seen. These cells were large with abundant granular cytoplasm in the specimen from the ovary. These cells were identified as decidual cells. The ovarian cyst was reported as ovarian deciduosis in permanent pathologic examination (Fig. 3).
Discussion
Decidual reaction is a well-documented physiological phenomenon of pregnancy which arises from a progesterone-induced metaplasia of subserosal stromal cells [3]. With increasing duration of pregnancy, there is vacuolar degeneration and fragmentation of the decidua cells as a manifestation of regressive changes. The involution of the decidua takes place in four to six weeks post partum [6]. In the absence of pregnancy, it has been considered that stimulation of appropriate cells by progesterone and progesterone-like substances from the corpus luteum or the adrenal cortex causes ectopic decidual formations [7,8]. It has been observed most often in the cervix and appendix [1,3]. Gross ovarian deciduosis is a rare lesion. The intraoperative appearance suggests mucinous cystadenoma.
Deciduosis is an incidental finding that has not been associated with clinical symptoms [3,9], however, rare life-threatening events have been reported [10]. Deciduosis is usually an incidental microscopic finding, detected in biopsies taken during caesarian sections, postpartum tubal ligations, appendectomies and in-tubal pregnancies [1]. The decidual cells on microscopy appear large with abundant cytoplasm and a bland nucleus.
We experienced an unusual case of ovarian deciduosis in a primigravida that was suspicious for ovarian malignant tumor. Though a rare event, it should be considered as a differential diagnosis in cases presenting as ovarian malignant tumor during pregnancy.

 XML Download
XML Download