

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Angiomyofibroblastoma (AMFB) was first described by Fletcher et al. [1] in 1992 as a well circumscribed, benign tumor that has histological similarity to aggressive angiomyxoma. Since then, only dozens of cases of AMFB of various sites have been reported worldwide. According to the cases of AMFB reported so far, it is understood that the major site of AMFB is the vulva of premenopausal women [2]. It is also known that AMFB can be found in the vagina, fallopian tube, perineum, and cervix in female, and scrotum, inguinal canal and spermatic cord in male [2]. The clinical presentation of most of the tumors reported consists of slowly-growing painless masses with low tendency for a local recurrence [3]. The lesions are well circumscribed and range from 0.5 to 12 cm in size [1]. Microscopically the tumors are characterized by alternating hypocellular and hypercellular areas composed of spindle and round shaped cells with numerous blood vessels. Immunohistochemically, the stromal cells show uniform positivity for vimentin and desmin [1-4]. Treatment is surgical excision [4].
Case Report
In 2011, a 43-year-old para 3 woman was referred to the gynecologic clinic of Jeju National University Hospital, presenting an asymptomatic mass of the vagina. The patient's medical history showed breast cancer in 2005, of which treatments included a partial mastectomy with axillary lymphadenectomy, adjuvant chemoradiotherapy, and tamoxifen therapy for 5 years. Postoperatively, the patient had also had regular pap smear tests and ultrasonography at a local clinic. The gynecological examination had been negative for 5 years. The mass was detected accidently during routine gynecological examination without any symptom. On palpation, the mass was noted about 3 cm in size, mobile, and rubbery with a short, narrow stalk arising from 9 o'clock direction of the uterine exocervix (Fig. 1). Consequently, the patient was diagnosed as a cervical myoma and underwent a local excision of the tumor. The postoperative course was uneventful.
1. Gross finding
The specimen was an oval soft tissue mass, 3×3×2.5 cm in dimension, partially covered by mucosa. On section, the cut surface appeared homogenous light yellow, and myxoid without evidence of necrosis or hemorrhage.
2. Microscopic finding
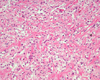
Light microscopic examination revealed that spindle or oval shaped tumor cells that were arranged around numerous thin-walled blood vessels in loose plump stroma (Fig. 2). The nuclei of the tumor cells were relatively uniform, bland-appearing with eosinophilic cytoplasm without mitotic figure or atypia.
3. Immunohistochemical finding
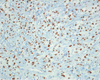
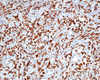
Immunohistochemically, the stromal tumor cells of AMFB showed strong positivity for desmin (Fig. 3) and vimentin. The staining for estrogen receptors and progesteron receptors was also positive (Fig. 4). But no immunoreactivity was detected for alpha-smooth muscle actin, CD34.
According to these findings, the tumor was finally diagnosed as a "angiomyofibroblastoma". No additional therapy was given.
Discussion
AMFB is a rare, benign, mesenchymal tumor of unknown pathogenesis, more likely involving the female lower genital tract. Only dozens of cases of AMFB have been reported worldwide and 7 domestic cases have been reported in South Korea since AMFB was first described by Fletcher at al. [1] Statistics show that 79% of AMFB were reported to occur in the vulva of postmenopausal women, 9% in the vagina, and the rest of 12% were reported to occur in the perineum, inguinal canal, fallopian tube, and cervix in female [2]. As the statistical data shows, AMFB of the cervix is quite rare; in fact, there is only 1 documented case in literature so far [2,5].
The pathogenesis of AMFB is not identified yet. However, the neoplastic cells of AMFB is suggested to arise from common mesenchymal cells within the specialized band of myxoid subepithelial stroma extending from the endocervix to the vulva [6]. This may explain the tendency for these tumors to occur in the lower female genital tract [7]. Immunohistochemically, the tumor shows positivity for hormonal receptor, therefore it is possible to assume that hormonal stimuli involved in neoplastic proliferation of mesenchymal cells. The fact that the tumor usually develops in premenopausal women also suggests that estrogenic stimuli might have an important role in the development of AMFB [8].
In breast cancer patients, it is generally known that tamoxifen treatment can increase the incidence of cervical and endometrial polyps, endometrial hyperplasia, ovarian cyst, endometriosis, adenomyosis, leiomyoma and endometrial carcinoma as a result of its estrogenic effect on the female genital tract. The incidence of uterine mesenchymal neoplasm can also be increased by tamoxifen therapy [9]. A case of angiomyofibroblastoma related to tamoxifen treatment in a breast cancer patient was first reported by Varras et al. [10] The author assumed that tamoxifen may exert hormonal stimuli upon mesenchymal cells, resulting in the development of AMFB. Lee et al. [11] presented a case of AMFB of vagina in a toremifene, a synthetic analogue of estrogen receptors, treated breast cancer patient. They suggested that toremifene treatment might have been causally related to the development of AMFB by the same reason of tamoxifen [11]. There is also a domestic case report on vaginal AMFB in a breast cancer patient under tamoxifen treatment for 2 years by Bae et al. [12]; however, the case study doesn't specify the relationship of Tamoxifen and AMFB.
In summary, AMFB is a rare, benign tumor of female lower genital tract. It is possible that hormonal stimuli might have a role in the development of AMFB. Furthermore, it is potential that tamoxifen might give stimuli on hormonally responsible mesenchymal cells, resulting in AMFB. However additional studies required to establish the causal association between tamoxifen and AMFB.

 XML Download
XML Download