

 PDF
PDF ePub
ePub Citation
Citation Print
Print


It has been reported that an ovarian dysgerminoma originates from the germ cell of the ovary. The name 'dysgerminoma' proposed by Meyer in 1931. Dysgerminoma was investigated histologically. Diagnosis was made on serum lactic dehydrogenase (LDH), alpha-fetoprotein (AFP), as a tumor maker and serum LDH was considered to be an indicator of therapeutic effects. Dysgerminoma is malignant and tends to occur in young women, though the incidence of pregnancy with dysgerminoma is extremely low. This paper presents a dysgerminoma which developed in a patient in the seventh week of pregnancy and performed conservative operation for preserving pregnancy with laparoscopy.
Case Report
A 33-year-old housewife, 3 gravida, 1 para pregnant woman was transferred for early pregnancy with Rt. ovarian tumor. Her menarche was at the age of 12 years and she has regular menstrual cycle of 28 days. The patient noticed a mass in her lower abdomen during her antenatal care and transferred to our hospital. At her first visiting, she was at the end of 7th week of pregnancy and she complains the emesis. Pelvic examinations disclosed that a soft goose-egg-sized uterus was associated with a hard tumor of infant's head-size at its front. She was diagnosed as being in the seventh week of pregnancy, and the co-existence of solid ovarian tumor was also suggested. She was admitted to the hospital. She was 165 cm tall and weighed 53 kg. Her blood pressure was 120/70 mm Hg and her pulse rate was 84/min. No abnormalities were seen on the general findings. In Laboratory tests, the blood was type B, Rh-positive. No abnormality was observed in hematological test results. β-human chorionic gonadotropin (hCG) was measured as 75929.15 mIU/mL. As regards blood chemistry, LDH was 408 U/L, AFP was 13,464 ng/mL, CA-125 was 57.20 U/mL, CA 19-9 was 13.50 U/mL, and carcinoembryonic antigen (CEA) was less than 0.50 ng/mL. There were no abnormalities in urinalysis, electrocardiogram, pulmonary or respiratory data. Ultrasonography revealed that the uterus was 7×8 cm in size and had a gestational sac (GS) in its center. At the posterior of the uterus, there was a shadow of mass measuring 10×11×14 cm. The mass had multilocular profiles with some solid parts, and its wall looked slightly thick (Fig. 1).
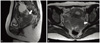
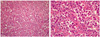
Pelvic magnetic resonance imaging (MRI) without enhance was performed. The mass mostly occupied the posterior pelvic cavity and impacted into the Douglas pouch as shown in Fig. 2. It measured a 5.8×9.8 cm in sized and was a lobulating contoured mass with intermediate signal intensity in T2 images. And a 4.3×3.3 cm sized cystic lesion was also observed. Its wall was sometimes thin and sometimes thick. On the basis of these findings, the mass was diagnosed as the granulosa cell tumor which occurred in the right ovary. Laparoscopic right adnexectomy and contralateral ovary biopsy were performed. About 10 cm sized and a relatively hard tumor with smooth surface was found in the median portion of Douglas pouch, slightly extended to the left of the pelvic cavity (Fig. 3). The tumor originated from left ovary. It was partly cystic but mostly solid. Microscopically the tumor cells have prominent cell membrane, abundant pale to granular cytoplasm and uniform nuclei having prominent nucleoli. In the fibrous stroma, variable amounts of chronic inflammatory cells especially lymphocytes are found. And occasional mitoses are found (Fig. 4).
Discussion
Pregnancy induces dynamic changes in endocrinological activity throughout the female lives. Therefore such assumption may not be always misdirected that various ovarian tumors, especially malignant tumors derived from germ cells, are apt to appear during pregnancy. However, a few cases of dysgerminoma associated with pregnancy have been reported up to now.
The rate of malignant tumors in the total number of ovarian tumors associated with pregnancy was reported from 1.3% to 7.9% [1]. In our clinic, the rate of malignancy was very rare as less than 1%. This is markedly lower than that of the patients without pregnancy. From these facts, it may be said that the rate of the malignant ovarian tumors associated with pregnancy is rather low. Beischer et al. [2] have explained that such differences in the rate of malignant ovarian tumor are caused by the difference in age distribution between non-pregnant and pregnant women. Most of the patients with malignant ovarian tumor were over 40 years old and those patients were rarely pregnant [2]. In our clinic, 62.2% of the patients with malignant ovarian tumor belonged to the group of 40 years old or more. Dysgerminoma is considered to be one of the most common ovarian tumors in reproductive age [3-5]. Fortunately it is rather rare but unfortunately the management for a gynecologist to encounter patients who have developed dysgerminoma during pregnancy has not well known.
How pregnancy influences dysgerminoma or how dysgerminoma influences pregnancy has been discussed. Bakri et al. [6] reported that the association of pure dysgerminoma and pregnancy did not adversely affect the tumor prognosis or fetal outcome. In our patient, neither clinical, histological nor cytological findings indicated that dysgerminoma were not influenced by pregnancy. Malignant ovarian tumors associated with pregnancy tend to progress asmyptomaticcally and there are no differences with benign ovarian tumors in early stages. Therefore, we are facing some difficulties in making a correct diagnosis of ovarian cancer in pregnancy. In some patients, they complained bearing down sense or pressure in the lower abdomen, when the ovarian tumors had grown up to some extent. But a huge gravid uterus makes pelvic examinations insufficient, and also it is impossible to conduct computed tomography (CT) scan. Occasional ultrasonography should be performed in order to confirm whether ovarian tumor is present or not. It is very useful to evaluate whether tumor is cystic or solid. In general, non-enhanced MRI is relatively accurate and recommended. The LDH value is hard to work as the indicator of malignant ovarian tumor when the patient is pregnant.
The treatment of ovarian malignant tumor with pregnancy is as difficult as the diagnosis. Because of the very few cases there's lack of statistically significant experience world-wide. Therefore debate is even further. Concerning the treatment of ovarian cancer, Disaia et al. [7] proposed the following eight conditions to conduct conservative operation; 1) cancer classified as stage Ia, 2) well differentiated mucinous, endometrioid or mesonephric histology 3) a young woman of low parity, 4) otherwise normal pelvis, 5) encapsulated and free of adhesions, 6) no invasion of capsule, lymphatics, or mesovarium, 7) peritoneal washings negative, 8) ovarian wedge biopsy and omental biopsy negative, and 9) close follow up. Munnell [8], and Graber and Barber [9] also indicated that when low grade mucinous cyst-adenocarcinoma, arrhenoblastoma, dysgerminoma, granulosa theca cell tumor or low grade papillary tumor is observed at its Stage Ia during pregnancy, the disease can be treated only by resection of an affected ovary.
In our case, we performed unilateral adnexectomy and contralateral ovarian biopsy. Grossly the tumor was confined within one ovary and its capsule was intact. In frozen biopsy of contralateral ovary and cytology was negative. We enveloped the tumor mass twice with endopouches and removed it out through the 12 mm trocha incision site which extended to 15 mm. During the operation tumor cells were not spilled. After operation we check the fetal health and the fetus had not any problem. We planned the post-operative follow-up with ultrasonography and LDH comparing with initial value. And non-enhanced pelvic MRI is also checked occasionally.
Our hospital also had no statistical data for treatment or prognosis of dysgerminoma during pregnancy. Especially whether it may have no problem to performed resection of affected side adnexae only or not. But in my opinion, after giving general information about dysgerminoma to parents conservative management may be enough in stage Ia dysgerminoma if they agree.


 XML Download
XML Download