

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Medulloblastomas are rare neoplasms in adults. Medulloblastomas are treated by surgical removal of the tumor followed by radiotherapy. Because craniospinal irradiation can damage the hypothalamic-pituitary axis, uterus, and ovaries, and consequently result in infertility, the probability of pregnancy is quite low. We managed a patient who had undergone resection of a posterior fossa medulloblastoma and received craniospinal irradiation, who conceived spontaneously during follow-up. She was diagnosed with a recurrent medulloblastoma with metastasis to the spine accompanied by headaches and back pain at 26 weeks gestation. Conservative treatment measures were utilized in an effort to prolong the pregnancy. She was delivered by cesarean section due to recurrent seizure activity at 29 weeks plus 3 days gestation. The neonate made favorable progress and was discharged in good condition.
Figures and Tables
Fig. 1
T2 weighted coronal MR image of brain shows high signal at the bilateral cerebellum and vermis. These findings are old leukoencephalomalatic changes with atrophic changes. Dark signal dot (white arrow) at the left cerebellum is suggested hemangioma.
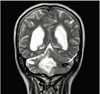
Fig. 2
(A) Fat suppressed T2 weighted sagittal MR image of spin shows a small nodular mass (white arrow) with high signal on dorsal portion of spinal cord at C7 level. (B) Multiple lesions (white arrow heads) are also seen along intradural and extramedullary layer on the thoracolumbar spine level. These masses surround and compress spinal cord, and extend along the cauda equina.

References
1. Seok JY, Kim SH, Lee YH, Kwon J, Kim TS. Vimentin and survivin expression rates as prognostic factors in medulloblastoma. Korean J Pathol. 2007. 41:87–94.
2. Chan AW, Tarbell NJ, Black PM, Louis DN, Frosch MP, Ancukiewicz M, et al. Adult medulloblastoma: prognostic factors and patterns of relapse. Neurosurgery. 2000. 47:623–631.
3. Fukunaga-Johnson N, Lee JH, Sandler HM, Robertson P, McNeil E, Goldwein JW. Patterns of failure following treatment for medulloblastoma: is it necessary to treat the entire posterior fossa? Int J Radiat Oncol Biol Phys. 1998. 42:143–146.
4. Friedberg MH, David O, Adelman LS, Heilman CB. Recurrence of medulloblastoma: violation of Collins' law after two decades. Surg Neurol. 1997. 47:571–574.
5. Wo JY, Viswanathan AN. Impact of radiotherapy on fertility, pregnancy, and neonatal outcomes in female cancer patients. Int J Radiat Oncol Biol Phys. 2009. 73:1304–1312.
6. Pai HH, Thornton A, Katznelson L, Finkelstein DM, Adams JA, Fullerton BC, et al. Hypothalamic/pituitary function following high-dose conformal radiotherapy to the base of skull: demonstration of a dose-effect relationship using dose-volume histogram analysis. Int J Radiat Oncol Biol Phys. 2001. 49:1079–1092.
7. Razak AR, Nasser Q, Morris P, Alcutt D, Grogan L. Medulloblastoma in two successive pregnancies. J Neurooncol. 2005. 73:89–90.
8. Stevenson CB, Thompson RC. The clinical management of intracranial neoplasms in pregnancy. Clin Obstet Gynecol. 2005. 48:24–37.
9. Chaudhuri P, Wallenburg HC. Brain tumors and pregnancy. Presentation of a case and a review of the literature. Eur J Obstet Gynecol Reprod Biol. 1980. 11:109–114.
10. Tewari KS, Cappuccini F, Asrat T, Flamm BL, Carpenter SE, Disaia PJ, et al. Obstetric emergencies precipitated by malignant brain tumors. Am J Obstet Gynecol. 2000. 182:1215–1221.
11. Shellock FG, Kanal E. SMRI Safety Committee. Policies, guidelines, and recommendations for MR imaging safety and patient management. J Magn Reson Imaging. 1991. 1:97–101.
12. Choi JU, Yoon KY, Han JM, Jung YA, Rhim CC, Kim SJ, et al. A case of maternal metastatic brain tumor was detected in midtrimester. Korean J Obstet Gynecol. 2006. 49:2388–2393.
13. Park IY, Yi CS, Shin JC, Lee JH, Lee HJ, Kang DH. Proper time of delivery to decrease minor perinatal morbiditles. Korean J Obstet Gynecol. 2002. 45:373–377.
14. Pollack RN, Pollak M, Rochon L. Pregnancy complicated by medulloblastoma with metastases to the placenta. Obstet Gynecol. 1993. 81:858–859.
15. Brossard J, Abish S, Bernstein ML, Baruchel S, Kovacs L, Pollack R. Maternal malignancy involving the products of conception: a report of malignant melanoma and medulloblastoma. Am J Pediatr Hematol Oncol. 1994. 16:380–383.
 XML Download
XML Download