

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Based on 2013 estimations of the World Health Organization, about one billion people worldwide were active smokers and around six million people died from diseases caused by smoking, including mainly cardiovascular and pulmonary diseases as well as cancer [1]. Epidemiological studies on upper tract urothelial carcinoma (UTUC) and urothelial carcinoma of the bladder (UCB) have identified several etiological risk factors, with cigarette smoking and exposure to certain occupational agents being of highest importance [234]. Out of the more than 60 carcinogens and free reactive oxygen radicals, the main relevant metabolites responsible for urothelial carcinoma (UC) development are not reliably identified yet; however, it is proven that smoking impairs cellular DNA repair mechanisms, which subsequently diminishes the body's defence mechanisms (host response) against carcinogens [45].
In 2013, 382,700 new cases of UCB were diagnosed worldwide and they were 143,000 associated deaths [16]. In half of UCB-patients smoking is the most relevant risk factor; while studies have shown that smoking cessation in UCB-patients significantly reduces the risk for recurrence [78910]. Based on the results of a recent meta-analysis of 83 studies, the relative risk for developing UCB was 2.58 (95% confidence interval [CI], 2.37 to 2.80) in all smokers, with active smokers having a relative risk of 3.47 (95% CI, 3.07 to 3.91) while the relative risk of former smokers was 2.04 (95% CI, 1.85 to 2.25) [1]. In addition, cancer-specific mortality was higher in smokers (active and previous smokers combined) by 47% (95% CI, 24% to 75%) [1].
Finally, there is an abundance of evidence that physicians should provide smoking prevention and cessation counselling in a prophylactic manner for promotion and maintenance of personal health. The time of UC diagnosis has been shown to be a “teachable moment,” highlighting an opportunity for urologists and oncologists to recommend rigorous smoking cessation to enhance the individual tumor-specific prognosis. To date, a paucity of data exists on the knowledge of UC-patients regarding the association of their tumor disease with smoking habits. Furthermore, limited studies have investigated which communication between doctors and patients on this critical point is undertaken in clinical routine and which resources and aids for smoking cessation are offered by physicians (and mainly urologists) to UC-patients who are active smokers. In a survey conducted at the Johns Hopkins Hospital in Baltimore by Guzzo et al. [11] on 71 UCB-patients only 84.5% were aware of smoking as a risk factor for UCB development and 59% of active and previous smokers were advised by their urologists to quit smoking or not to restart again. Studies on this topic conducted in Europe are yet pending.
The aim of the present bicentric survey study was to analyze knowledge and awareness level of UC-patients concerning the association of their tumor disease with smoking. Furthermore, we aimed to evaluate the association of smoking habits and tumor stage. Based on the analysis of available services for smoking cessation and the time volume of accordant informative conversations, also the status quo concerning current implementation of elementary and selffinancing conversations of physicians with their patients will be displayed.
Go to : 
MATERIALS AND METHODS
1. Study conduction
A survey comprising 23 items was developed with the aim of assessing knowledge and awareness level of in-house patients with a histologically confirmed genitourinary malignancy (UTUC, UCB, renal, prostate, and testicular cancer) on the association of their tumor disease (and other urological tumors) and cigarette smoking (concerning tumor development and prognosis). Selective questions were integrated to assess 1) the manner and the extent of medical informative conversations conducted in this regard and 2) the resources provided to patients for smoking interruption or cessation. Previous smokers were asked for their individual reasons that had led them to quit smoking, and current smokers were queried for their concrete further intention regarding cigarette consumption. Prior to study initiation the survey was validated on 25 patients with uro-oncological diseases to confirm comprehensibility and clarity of questions. Study inclusion criteria were histologic confirmation of a urologic malignancy, the capability of informed consent, and an age of at least 18 years. The study title was defined as “Knowledge of tumor patients regarding the Risk Association of smoking habits and Urological Tumors” (KRAUT study); ethical committee approval of the State Chamber of Medicine in Brandenburg was obtained (BLAEK-EK no. 13012). Written informed consent was obtained from all patients before enrolment. The study was conducted between September 1st 2013 and December 31st 2014 in two urological departments (Caritas St. Josef Medical Center, University of Regensburg; St. Elisabeth Hospital Straubing; Academic Teaching Hospital of TU Munich University) [1213]. In addition to the 23 items of the survey, demographic, clinical, and oncological information was obtained from all enrolled 258 patients (UC, n=88; renal cancer, n=34; prostate cancer, n=124; testicular cancer, n=12).
2. Study group and study criteria
The study group comprised 88 patients with histologically confirmed UC (UCB, n=85; UTUC, n=3), who underwent inhouse treatment in two urological departments (Straubing, n=42; Regensburg, n=46). During the assessment period 256 (76+180) UC-patients (coded as C65–67) were treated with an in-house duration of >1 day, so that overall 34.4% of possible patients could be included. They study survey is shown in the Supplementary material. Patient related criteria included age, gender, body mass index (BMI), and tumor manifestation (within three months since diagnosis versus tumor recurrence). Furthermore, clinical-pathological tumor stage was assessed in a dichotomized manner (<c/pT2, c/pN0, c/pM0 vs. muscle-invasive and/or metastasized tumor stages).
3. Statistical analysis
Continuous variables are displayed with medians and interquartile ranges (IQR). To analyze differences in the distribution of continuous parameters between non-smokers and smokers (summarized as active and previous smokers), the Kruskal-Wallis-H Test was applied. The distribution of categorical variables in different groups was compared by chi-square test. If reasonable, descriptive results of nominal scaled items were displayed in summary. Two multivariate logistic regression models (MLRM) were built to assess the independent impact of smoking as dependent dichotomized variables on tumor stage with one model adjusted for the smoking status variable and the second model including the number of pack-years.
The preferable sample size to achieve a statistical power of 0.8 to 0.85 for this study was neither reached a priori nor post-hoc, as no information was available on the putative effect size for the impact of smoking on the binary categorized tumor stage (see above). This information would have potentially been extractable for cancer-specific mortality analyses from recent meta-analyses; however, for the advised surrogacy analyses of the present study (comparison of tumor stages) this information was not provable [19].
For data analysis IBM SPSS Statistics ver. 24.0 (IBM Co., Armonk, NY, USA) was applied. The p-values provided are two-sided with a level of significance defined as p<0.05 for all tests conducted.
Go to :
RESULTS
Eighty-eight UC-patients (85 and 3 with UCB and UTUC, respectively) were enrolled in the study, of which 23 (26.1%), 41 (46.6%), and 24 (27.3%), respectively, were nonsmokers, previous smokers, and active smokers. Descriptive patient characteristics and comparison between nonsmokers and smokers are displayed in Table 1. The median age of the study group was 69 years (IQR, 61 to 73.8) with no significant difference between non-smokers and (active as well as previous) smokers (p=0.102). The median age of active and previous smokers was significantly different (64 years vs. 70 years, p=0.002), while there was no significant difference in the median number of pack-years between both groups (29.3 vs. 29.2, p=0.946). Forty-nine patients (55.7%) had a primary UC at the time of study conduction (initial or subsequent treatment within three months of diagnosis), 18 patients (20.5%) presented with muscle invasive and/or metastatic disease.
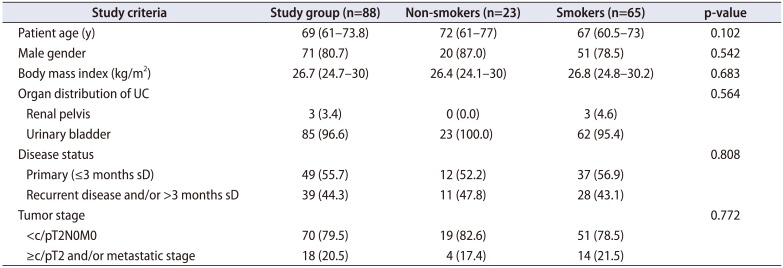
Table 1
Distribution of clinical and oncological criteria in 88 patients with UC of the renal pelvis or bladder, distributed in non-smokers and smokers (active and previous smokers)
![]()
Exactly 64.9% of patients who responded to these questions (50/77) considered it possible that cigarette consumption could generally impact UCB development. Forty of 67 patients (59.7%) considered it as conceivable or proven that cigarette consumption impacts UCB prognosis. In comparison, 100% of patients who responded to both questions considered the impact of smoking on the development and/or prognosis of bronchial carcinoma as probable or proven. There was a significant agreement in the judgement of those patients, who estimated the impact of smoking on UC development and prognosis as possible or proven (p<0.001).
Exactly 32.3% of smokers (21/65) confirmed to have altered their cigarette consumption due to their tumor disease. Ten of these 21 patients had quit smoking after UC diagnosis, furthermore 11 had reduced consumption. Additionally, 31 patients had stopped smoking for various reasons unrelated to their tumor disease. Fifteen of 24 active smokers (62.5%) confirmed that they would have stopped smoking immediately if they had known about a possible association with UC development and prognosis. Only six of 24 active smokers (25.0%) and 10 of 41 previous smokers (24.4%) considered smoking the main cause of UC development.
Eight of 24 active smokers (33.3%) had been directly advised by their treating physicians to quit smoking due to their tumor disease and of 41 previous smokers, 12 patients (29.3%) had received a clear recommendation by their physician(s) to stop smoking due to their tumor disease or to not restart smoking again. Ten of 24 active smokers (41.7%), 17 of 41 previous smokers (41.5%) and 5 of 23 nonsmokers (21.7%) had an accordant informative conversation with their urologist concerning the association of cigarette consumption and UC prognosis (further 8.3%, 7.3% and 4.3%, respectively, received this information exclusively by physicians from other medical specialties). On the other hand, of 24 active and 41 previous smokers 7 (29.2%) and 13 (31.7%) patients indicated that they don't require an informative conversation with physicians or don't consider such conversation as necessary. Seven active smokers (29.2%) and 2 previous smokers (4.9%) had been offered services for smoking cessation. Nine patients only of the entire study group (10.2%) indicated that the cumulative time used for accordant informative conversations on the association of cigarette smoking with urological tumor diseases comprised 10 minutes or more.
Exactly 17.4% (4/23), 24.4% (10/41), and 16.7% (4/24) of nonsmokers, previous smokers, and active smokers, respectively, presented with muscle-invasive and/or metastatic disease (group comparison, p=0.772). Both smoking anamnesis (odds ratio [OR], 1.46; p=0.574) and cumulative dose/pack-years (OR, 1.00; p=0.912) didn't have an independent impact on tumor stage (Table 2). BMI had a significant impact on this endpoint with every increase in BMI per kg/m2 reducing the possibility of muscle-invasion and/or metastatic tumor stage by 18% (95% CI, 4% to 29%; p=0.012) (Table 2, Fig. 1).

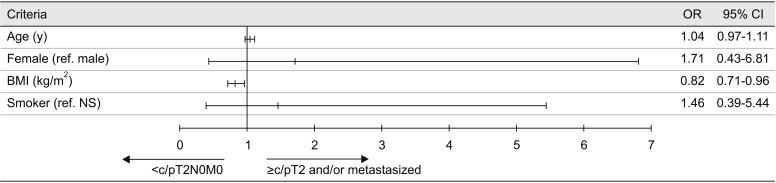 | Fig. 1Results of multivariate regression analysis for the impact of smoking status (active or previous smokers vs. non-smoker) on tumor stage (presence of muscle-invasive and/or metastatic urothelial carcinoma). OR, odds ratio; CI, confidence interval; BMI, body mass index; ref., reference; NS, non-smoker.
|
Table 2
Multivariate logistic regression model to evaluate the independent impact of different criteria on the presences of muscle-invasive and/or metastatic disease
![]()
Go to :
DISCUSSION
Health care providers are urged to advise their patient population about the significant impact of smoking on cancer development and the associated increase of cardiovascular and pulmonary morbidity and mortality. Programs and initiatives to increase the awareness in this regard should aim to counsel non-smokers to maintain their abstinence and to recommend smokers to quit smoking. Besides impairment of different organ functions (and subsequently potentially also the individual capability for surgery and anaesthesia), smoking contributes to UC, renal, and penile cancer development as well as impacts prognosis of UC and prostate cancer patients [1415]. For UC (especially UCB) the evidence is consistent and reliable: smoking represents the main risk factor for cancer development and is additionally associated with an impairment of the cancer-specific prognosis [12345678910]. Furthermore, the association between smoking duration and intensity with erectile dysfunction is clearly proven [16]. Taken together, these smoking related genitourinary diseases place the urologist in a unique position to provide smoking cessation guidance.
Which conclusions should urologists draw by the abovementioned insights and the results of our survey? About 74% of study participants with histologically confirmed UC were active or previous smokers; for both groups of smokers about 30 pack-years were calculated on average with no significant difference between both groups. Although 50% of patients who were active smokers at the time of diagnosis had a conversation with their physician(s) about the correlation of their tumor disease with smoking, only 25% were aware of smoking as main risk factor of UC development. One third of active smokers only were directly asked by their physicians to quit smoking and 42% of patients belonging to this group were informed that maintenance of smoking could result in a tumor-specific impairment of their prognosis. 29% of active smokers and 5% of previous smokers only were offered support for smoking cessation by their physicians during their active smoking period. Also, only 10% of the entire study group had informative and educational conversations about the potential negative impact of smoking of cumulatively at least 10 minutes. Based on the results of this survey, it appears that urologists inadequately communicate (as it concerns time and content) with UC-patients about the adverse impact of smoking. Further studies have confirmed this observation and indicate a need for optimization in this regard on a worldwide level [111718192021]. In a study by Bjurlin et al. [18] on 535 in-house urological patients with different diseases 25% of patients considered smoking as relevant for UCB development. The study results published by Westhoff et al. [19] on 1,735 long-term survivors with UCB recorded in the Netherlands Cancer Registry between 2007 and 2012 even showed that only 10% considered smoking as causative for UCB development. In a 2013 national survey of urologists, Bjurlin et al. [22] indicated that urologists have the responsibility to counsel their patients by structured education and provision of specific support for smoking cessation to strictly quit smoking. How this “teachable moment” at the time of cancer diagnosis could be used to motivate patients to completely change their lifestyle (including smoking reduction or cessation) has been addressed by a structured program introduced by Lee et al. [23]. In this regard, urologists should also be aware of their function as primary contact for UC-patients and should aim to extend their core competence in diagnostics and treatment of this disease also to aspects of lifestyle changes impacting the course of disease.
Based on the results of our study we could not confirm an association between cigarette smoking and the presence of advanced tumor stages. 17.4% and 21.5%, respectively, of non-smokers and (active and previous) smokers had a tumor stage >c/pT1N0M0 (p=0.772). Based on two multivariable models neither smoking status (smoker vs. non-smoker) nor the cumulative smoking dose (based on pack-years) had an independent impact on tumor stage. Also, when this category was adapted (e.g., >c/pTaN0M0), smoking status and cumulative dose didn't significantly impact this endpoint (results not shown). In contrast, larger studies with better definition of advanced UC stages could show an association with smoking and more aggressive tumors [2425]. Interestingly, in the present study, BMI was the only criterion significantly impacting tumor stage, while every increase in BMI per kg/m2 reduced the risk of a muscleinvasive and/or metastasized tumor stage by 18% (p=0.012). The international evidence is inconsistent in this regard, however, the association between a higher BMI and less advanced tumor stages has been described by other work groups as well [2627].
Several limitations concerning the interpretation of our study need to be considered. In addition to the overall limited number of patients participating in this survey, only 34.4% of possible UC-patients could be included. This is remarkable, as this selection bias (participants vs. responders) could potentially also impact results; furthermore, potentially significant differences could fail due to limited statistical power (see also MATERIALS AND METHODS section). Since the KRAUT study was developed for urological cancer patients in general, but not specifically for UC-patients, clinical and oncological criteria gathered in the survey population represent a compromise to cover different urological tumors; desired UC specific criteria (treatment modalities) and general criteria (occupational exposure, educational status, assignment to different referring medical specialties) were not collated. Due to the lack of validated questions in this specific setting, the items of this study were self-designed. However, prior to study start, all survey questions were validated in structured interviews with 25 uro-oncological patients in one hospital (St. Elisabeth Hospital Straubing, Germany). Furthermore, this study was conducted as a survey, hence, honesty of patients concerning their smoking habits is desired, but not a precondition which can be postulated. In addition, not all items were responded by all patients (whereas all questionnaires were controlled for plausibility by both data responsible persons [MD, OM] together. Based on the evaluated questions, we could not generate findings about secondary smoking exposure, which could impact study results (especially in cases of long-term exposition). Patients included in the KRAUT study were not further followed for their oncological course.
Go to :
CONCLUSIONS
The knowledge of UC-patients concerning the general association of their tumor disease with smoking seems to be limited. Comparable to other tobacco associated cancers, the time of UC diagnosis may allow physicians to use this time-point as a “teachable moment” in order to educate patients in a structured manner and to offer active smokers sufficient support for smoking cessation. Urologists remain in a unique position and should actively counsel patients concerning possible lifestyle changes, ultimately strengthening their role as primary partners of UC-patients in the comprehensive therapeutic management of UC.
Go to :

 XML Download
XML Download