

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In recent times, numerous pediatric surgical procedures have been adapted to less invasive approaches. Technological advances and increased surgeon training have paved the way for increased popularity worldwide. However, application of these techniques may be limited at times by factors such as pediatric body habitus. Body surface area (BSA) dictates the available landscape for laparoscopic port placement and instrument mobility. In pediatric urology, this is particularly relevant to minimally-invasive renal and ureteral surgery.
Trends in utilization of minimally-invasive pediatric urologic surgery are an ever-growing area of interest [1]. In 2005, the American College of Surgeons (ACS) collaborated with the American Pediatric Surgical Association to develop the ACS National Surgical Quality Improvement Program Pediatrics (NSQIP Peds) [23]. This is a prospectively collected database of voluntarily submitted cases performed in patients under the age of 18. It is currently drawn from over 100 sites, with each site required to have a full-time trained clinical reviewer. Preoperative and perioperative data, as well as 30-day complication rates are catalogued across most pediatric surgical subspecialties, including urology. Although the data has been well-studied in disciplines such as otolaryngology [4], plastic surgery [5], general surgery [6], neurosurgery [7], and orthopedics [8], efforts within urology have been limited [9101112].
Given the growth in both interest and performance of minimally-invasive variants of pediatric urologic procedures, we aimed to evaluate the difference in 30-day complications following commonly performed renal and ureteral surgeries, with comparison to those accomplished via open surgery.
Go to : 
MATERIALS AND METHODS
A retrospective cross-sectional analysis of data from surgical cases contained within NSQIP Peds was performed. Per our institutional policy, Institutional Review Board approval is not required for quality improvement review of the NSQIP databases. Cases of ureteroneocystostomy (UNC), pyeloplasty, complete and partial nephrectomy (PN) were identified using CPT procedure codes (Table 1). All cases for 2014 were identified and postoperative complications were examined. After examining baseline demographic data, we created receiver operator curves (ROCs) as predictor models for determining laparoscopic versus open approach. We then reviewed quality metrics of operative time, length of hospital stay (LOS), and 30-day complication rates for deep and superficial wound infections, urinary tract infections (UTIs), bleeding, and unplanned reoperation or readmission and compared between approaches. All comparisons were done using one-way ANOVA. All statistical analysis was completed using IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA).
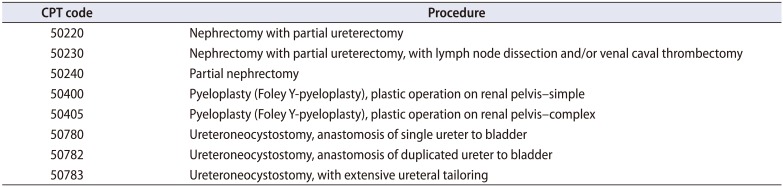
Table 1
Procedures and CPT codes
![]()
Go to :
RESULTS
There were 98 and 109 instances of open and minimally-invasive surgery (MIS) for nephrectomy, respectively. Patients undergoing open surgery had a mean age of 1,362 days, and a mean BSA of 0.45 m2, whereas those managed with MIS had a mean age of 1,956 days (p=0.012), and a mean BSA of 0.57 m2 (p=0.004). MIS was associated with longer operative time, with a mean time of 200 minutes for minimally-invasive nephrectomy compared to 132 minutes with the open approach (p<0.001). There was no significant difference in LOS, or rates of wound infections, pneumonia, bleeding/transfusion requirements, pulmonary embolism, UTI, sepsis, death, or readmission.
Regarding PN, there were 48 and 24 instances of open surgery and MIS, respectively. Overall, we found no significant difference in age between open and MIS (1,267 vs. 2,174 days, respectively), but there was a trend towards older children undergoing MIS (p=0.053). There was no significant difference in mean BSA by approach (0.46 m2 vs. 0.57 m2 for open and MIS, respectively; p=0.16). Mean operative duration was essentially equal between groups (185 vs. 189 minutes for open and MIS, respectively; p=0.88). However, LOS was significantly longer following open surgery (3.17 vs. 1.79 days, p=0.001). Comparisons among all other 30-day complication rates found no significant differences.
Review of instances of UNC noted 803 open and 117 MIS cases. Mean age was not significantly different between groups (1,631 vs. 1,679 days for open and MIS, respectively; p=0.72). Likewise, BSA was similar (0.50 m2 vs. 0.52 m2 for open and MIS, respectively; p=0.44). However, MIS took significantly longer (181 vs. 157 minutes, p=0.002). LOS did not reach significance (2.21 vs. 3.26 days for open and MIS, respectively; p=0.061). Comparisons among all other 30-day complication rates found no significant differences.
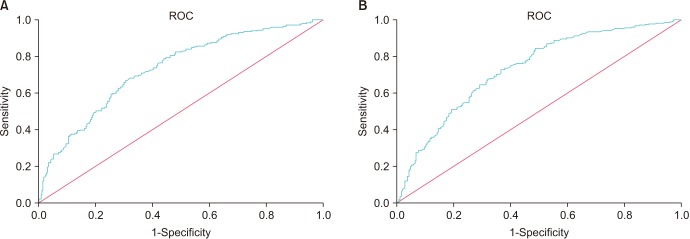
There were 349 and 276 cases of open and MIS pyeloplasty, respectively. Children undergoing MIS for this indication were significantly older (2,428 vs. 1,113 days, p<0.001). Correspondingly, recipients of MIS had a larger mean BSA (0.64 m2 vs. 0.40 m2, p<0.001). Using ROC for BSA, the AUC was found to be 0.730 and was significant (Fig. 1A). Children with BSA greater than 0.408 m2 were more likely to have MIS for pyeloplasty, with a sensitivity of 66.9% and a specificity of 69.3%. In terms of age, the AUC was 0.732 (Fig. 1B). Children older than 637.5 days were more likely to have MIS for pyeloplasty with a sensitivity of 72.8% and a specificity of 63.3%. MIS for pyeloplasty required longer operative time (203 vs. 142 minutes, p<0.001). LOS was similar (1.93 vs. 1.19 days for open and MIS, respectively; p=0.065). Comparisons among all other 30-day complication rates found no significant differences.
Comparative results are summarized in Table 2. The rate of superficial and deep wound infections, UTI, bleeding requiring transfusion, pneumonia, and readmission within 30 days was below 0.1% for all queried operations regardless of approach, with no significant differences between approaches in any of these metrics.
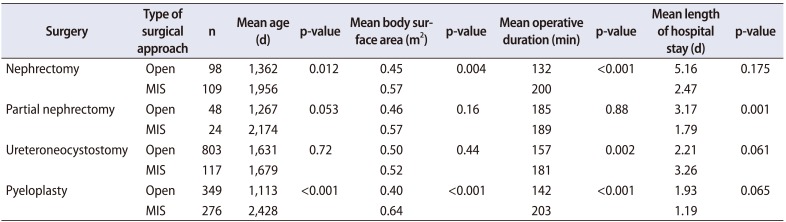
Table 2
Comparison of open and MIS variants of common pediatric urologic surgeries
![]()
Go to :
DISCUSSION
Numerous reasons are offered to support the increasing transition to MIS. These include, but are not limited to, improved cosmesis, increased intraoperative visualization, and elimination of human tremor with robotic assistance [13]. Incorporation of a surgical robot adds cost relative to conventional laparoscopy and open surgery, such that understanding outcomes is important [14]. This analysis pooled laparoscopic approaches and found that, compared to open surgery, there is no significant advantage in 30-day complications for the operations selected. However, this does not attest to long-term outcomes and cannot be used alone to dictate practice. Efforts such as this must be considered alongside other clinical data to determine the best approach for pediatric patients and the overall healthcare system. Open surgery was only associated with longer LOS for PN. Apart from PN, however, all operations performed via MIS demanded longer operative time than the open surgical approach.
This analysis offers some insight into patient selection. Not unexpectedly, the MIS appears to be increasingly applied to larger/older patients, presumably related to logistics of port placement and maneuverability of instruments with adequate field exposure. Those children managed with MIS for nephrectomy or pyeloplasty were significantly older, with a trend towards significance in PN cases. Similarly, those selected for MIS nephrectomy and pyeloplasty had significantly greater BSA. Again, since BSA increases with age, this is not surprising.
The transition point at which pediatric patients are more likely to undergo a MIS relative to an open approach for a given operation has not been previously reported. The ROC curves for pyeloplasty in this study found that children with BSA >0.408 m2 or age >637.5 days are more likely to receive MIS. The AUC was 0.730 and 0.732, respectively. While these transition points are not definitive and have low sensitivities and specificities, they offer a reasonable estimate, and may be useful in better understanding surgeon decision-making and comparing outcomes. Such information may also guide future instrument development by industry.
Prior evaluations of NSQIP Peds within urology have been limited. One prior study by Wang et al. [15] reviewed data on UNC alone, and included data from 1998–2012. Unlike our analysis, which focused on more contemporary data alone, they found that patients undergoing MIS UNC were more likely to be older and with a significantly higher rate of 30-day complications. In their work, however, the number of open cases was nearly 100 times higher than those managed with MIS. It is possible that limiting the analysis to more recent data provides better insight into current trends.
It was previously shown that increased specialization results in lower rates of complications and mortality [19]. While rates of overall 30-day complications following urologic surgery in children have been reported as low as 5.9%, cases involving urinary diversion and incorporation of bowel have been associated with rates as high as 27.8% [101216]. Adverse events in this early postoperative period seem to be more common among children managed at low-volume centers, especially in cases such as nephrectomy and percutaneous nephrolithotomy [17]. One analysis of NSQIP Peds data found that increasing body mass index (BMI) was a significant risk factor for post-operative events [18]. This may serve to highlight the difference in BMI and BSA, as the latter was significantly different between select groups in our study, but without increased risk of 30-day complications.
As with any retrospective database review, this study is not without limitations. This database provides no information regarding quality of life factors related to the improved cosmesis of MIS nor does it provide pain scale assessments of these patients postoperatively. The data is subject to human error in collection. Also, there is no information on long-term clinical outcomes. Additionally, this study of fers no insight into cost, which is of considerable interest to providers. Laparoscopic cases were viewed collectively regardless of robotic assistance. Thus, if the future trend is towards a different balance between conventional and robotic-assisted laparoscopy, repeat analysis may be indicated.
Go to :
CONCLUSIONS
Compared to open surgery, MIS for pediatric instances of nephrectomy, PN, UNC, and pyeloplasty demonstrated no difference in 30-day complication rates. We have determined contemporary thresholds for MIS based on patient age and BSA, which may offer insight into patient-selection by surgeons and subjective impressions of feasibility of MIS relative to patient factors. This information may be useful for future developments in surgical instrumentation. Data on short-term complications such as we've presented should be considered along future cost-analyses and reports of long-term clinical outcomes to better understand and ultimately dictate optimal application of technology relative to patient care.
Go to :
 XML Download
XML Download