

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cryopreservation of sperm was first established in the 1950s, with the first pregnancy achieved using frozen-thawed sperm reported in 1953 [1]. Initially, the use was limited to intrauterine insemination (IUI) and the post-thaw quality was often poor [2]. However, with the introduction of more sophisticated assisted reproductive techniques (ART), including in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI) within the last several decades, the issues with sperm quality and numbers of available motile sperm after thaw have, for the most part, been overcome. Now, cryopreservation of semen is widely used. Indications for storage commonly include diagnosis of cancer, as chemotherapies and radiation treatments may have deleterious effects on sperm production; men who wish to cryopreserve before proceeding with fertility treatments; and men who may be absent at critical points and unable to provide fresh sperm for ART [3].
The andrology lab at our institution has been offering cryopreservation services since the 1980s. The objective of this study was to examine the utilization and success for cryopreserved lots of sperm cells processed for men seeking this service at our multispecialty clinic in central Texas during the interval from 1988 through 2015 based on the indication for storage. Unique to our facility is that cryopreservation is offered for the purpose of military deployment for infertile couples who wish to continue treatments while the male partner is away or for men who were concerned about exposures during deployment.
Go to : 
MATERIALS AND METHODS
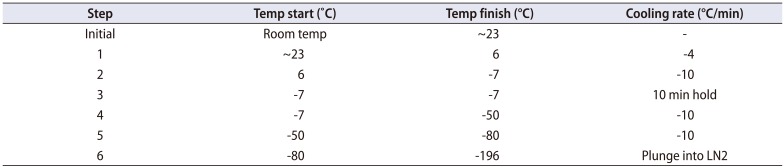
After Institutional Review Board approval was obtained through Scott and White Medical Center (approval number: 160447), a retrospective chart review was undertaken of all the cryopreserved semen samples at our institution from 1988 to 2015. The purpose for cryopreservation and eventual utilization of the sample were recorded along with outcomes of use for insemination, including cycles performed and clinical pregnancy. Semen samples were obtained via either ejaculation or surgical extraction after a sperm cryopreservation and storage agreement was signed by the depositor and a witness. The sperm were then frozen following a standard cryopreservation protocol. Each semen specimen was first washed via centrifugation with media containing antibiotics. The supernatant was removed and mixed with freezing media before insertion into labeled cryovials containing either 0.5 mL or 1.0 mL aliquots. The vials were then placed in a control rate freezer before ultimately being plunged into liquid nitrogen. See Table 1 for freezing schedule program.
For thawing, the samples were brought rapidly to 37℃ and diluted in culture medium before being centrifuged for 10 minutes. The supernatant was removed, and the sperm pellet was diluted in culture medium to the appropriate volume.
The types of utilization were accumulated as proportions for different purposes. The timing for use for insemination procedures was evaluated using Kaplan-Meier survival statistics with Gehan-Wilcoxon test to compare groups. The frequency of patients arranging to destroy samples was also reported and compared using a chi-square test. A p-value <0.05 was taken as significant.
Go to :
RESULTS
A total of 1,361 cryopreserved semen samples and 81 testicular or epididymal tissue samples were identified. Samples were cryopreserved for 1 of 4 purposes: ART focused on IUI, ART treatments incorporating IVF or ICSI, fertility preservation related to cancer treatment, or prior to military deployment (Table 2). Samples cryopreserved for IUI had the greatest usage rate at 64.3%. The greatest number of samples destroyed were those preserved to use as a backup for cycles of IVF or ICSI (251, 29.8%). A Kaplan-Meier plot illustrating the “utilization-survival” of cryopreserved sperm samples over time is shown in Fig. 1, where the y-axis represents the number of unused samples remaining cryopreserved at Scott and White Medical Center. As demonstrated in the plot, most utilization, regardless of indication for storage, occurs within the first year. The samples cryopreserved for male cancer patients had the highest proportion left in storage at 10 years, while the IUI samples had the lowest.

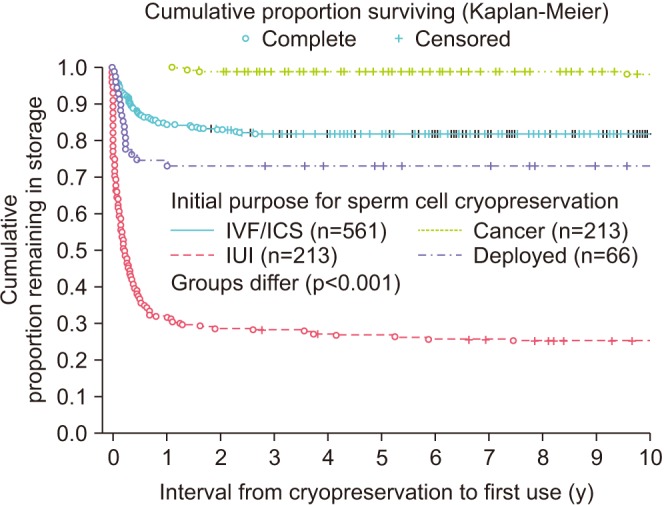 | Fig. 1Proportion of unused samples remaining in storage at our institution. IVF, in vitro fertilization; ICSI, intracytoplasmic sperm injection; IUI, intrauterine insemination.
|
Table 2
Cryopreserved semen utilization data
![]()
Including all indications, the total number of clinical pregnancies resulting from the use of cryopreserved samples was 51 for 210 cycles (Table 3). The highest success rate was with samples preserved for IVF/ICSI at 35.4% (34/96), and the lowest was 9.8% for IUI (14/143). Samples cryopreserved prior to deployment had a utilization rate of 22.8%, and these samples tended to be used within the first year of storage. The longest interval that a sample was cryopreserved before use resulting in a clinical pregnancy was 2.7 years.
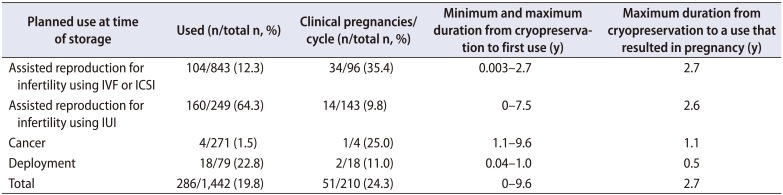
Table 3
Use of cryopreserved sperm cells for pregnancy: planned use at the time of storage and outcomes
![]()
Go to :
DISCUSSION
Sperm cryopreservation programs provide temporarily or permanently infertile men an opportunity to seek paternity in a timely fashion. With increased awareness of such programs among patients and providers, usage has steadily increased at many institutions [4]. Further, as fertility-related struggles can cause great distress for couples, psychological benefits to the availability of this service have been documented [56]. One group noted that 96% of men from a cancer cohort would recommend sperm cryopreservation to other patients [5]. Furthermore, the cost of sperm banking is usually not prohibitive with a median cost of 358 United States dollar (USD) and an annual fee storage fee of 244 USD [7].
Despite these factors, sperm cryopreservation programs remain underutilized. One survey found that, although the majority of oncology fellows and staff believe that sperm banking should be offered, approximately half noted that they either never brought up the topic or discussed it with fewer than a quarter of their eligible male patients [8]. Another study found during an 8-year interval, fewer than 9% of all men aged 18 to 55 were offered a fertility preservation consultation [9].
While similar statistics were not available at our institution, the data do likely reflect this trend toward limited utilization. Only 271 samples were cryopreserved for oncofertility during a 27-year interval within a multispecialty clinic with full spectrum oncology programs, including oncology fellowships. Over the same time interval, there were 3,050 diagnosed cancers in males aged 18 to 50, for a rate of approximately 8.9%. For comparison, in another large US-based series, 423 men preserved semen secondary to cancer during a 19-year interval from 1991 to 2010 [10]. In another, 306 out of 4,881 (6.3%) men aged 18 to 55 diagnosed with cancer underwent cryopreservation from 2002–2010 [9]. However, at our institution only 4 (1.5%) samples were used by cancer patients, below other reports of 5% to 10% utilization from US institutions [91011].
This low usage rate may be accounted for by several factors. For one, despite the cytotoxic nature of many cancer treatments, a large percentage of these men will have resumption of spermiogenesis. In fact, several reports demonstrate natural conception rates ranging from 23% to 47% in this cohort [71213]. Additionally, many young men simply may not be prepared to start a family following their bouts with cancer. One study demonstrated that only 10 out of 64 men (15.6%), including 56 who were less than 30 years old, had even attempted to achieve pregnancy following treatment [14]. Regardless, the psychological benefits of cryopreservation as described above and the risk of permanent subfertility in these patients highlight the need for increased awareness of the sperm cryopreservation service, both at our institution and elsewhere.
The vast majority of our samples were stored for purposes of infertility, specifically 843 (58.4%) for IVF/ICSI and 249 (17.3%) for IUI. Cryopreserved sperm can be used for multiple timed artificial-insemination attempts to improve the likelihood of conceiving, which may also be affected by the timing of the attempt of insemination, the location of sperm placement in the reproductive tract, and the quality of the sperm [15]. Furthermore, pooling samples from a single donor can increase the number of motile sperm in oligospermic males with which to attempt ART [16]. At our institution, the IUI samples had the highest rate of utilization (64.3%). However, pregnancy success rates were greatest for IVF/ICSI (35.4%). In one recent meta-analysis of reproductive outcomes in males with cancer using cryopreserved sperm, the fecundity rates using IUI and IVF were approximately 13% and 30%, which compare favorably with our results [17].
It is interesting to consider why the samples cryopreserved for purposes of IUI were more likely to be used and less likely to be destroyed than those for IVF/ICSI. One possible explanation is that the higher success rates of IVF/ICSI obviated the need for further utilization and storage. Another factor is the cost disparity of these procedures. A recent study demonstrated that couples using IVF had to pay a median of $19,234 for the first cycle and $6,955 for subsequent IVF cycles, while for IUI the median out of pocket costs were only $2,623 per cycle [18].
Given our institution's proximity to a large army base during a time of overseas deployment to address conflicts that have potential for toxic exposures, injury, or death, one unique aspect of our data are those samples cryopreserved for the indication of deployment. Frequently, cryopreservation supported infertile couples who wished to continue treatments while the male partner was deployed. Subsequently, the samples stored for this purpose tended to be utilized relatively frequently (22.8%) and quickly, as all utilized samples were used within 1 year of storage. Male patients do have a risk dying while deployed, which brings up the question of posthumous sperm utilization. In a recent survey by Pastuszak et al. [19], 87% of infertile men reported that they would consent to posthumous utilization of their sperm. Regardless, this practice remains controversial, and it highlights the importance of a thorough discussion and informed consent with these couples prior to cryopreservation.
Limitations to our study include its retrospective nature and lack of data on semen parameters. Its strengths include a large time period and sample size. Furthermore, as mentioned above, the deployment cohort has not been previously described in the literature.
Go to :
CONCLUSIONS
In conclusion, sperm cryopreservation is a valuable service that has dramatically aided assisted reproduction techniques over the last half century with a variety of indications for storage, including military deployment. Our study not only provides further support for the role and utilization of cryopreserved sperm in infertility treatments but also highlights the need for education and awareness of the benefits of such a program, especially amongst male cancer patients.
Go to :
 XML Download
XML Download