

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The transvaginal mesh (TVM) reconstruction procedure for vaginal prolapse, in which synthetic mesh biomaterials are implanted in a transvaginal operation, first appeared in 2000 as a method to support the pelvic organs with stronger and more ideal forces, the main surgical treatment for pelvic organ prolapse (POP) underwent a dramatic change [1]. Actually, the rates of recurrence in the first year after surgery with TVM were around 10%, and the results were often reported to be much more satisfactory than those for conventional native tissue repair [23]. Thus, the TVM procedure instantly spread around the world. In 2010, 10 years after the first report, as many as approximately 75,000 TVM operations were performed. Now, standardized surgical kits are marketed all over the world, and the operative method has become standardized. Unfortunately, however, these commercial kits for mesh prolapse surgery have not received governmental approval in Japan.
In many Japanese institutions, as a last resort, the surgeons personally create a mesh insert to use for the operation by cutting soft polypropylene mesh to match the pattern of the Prolift System (Ethicon, Somerville, NJ, USA) that is used in Europe and America. In addition, the operation has been performed by means of passing the arms of the cut mesh through the obturator foramen and sacrospinous ligament (SSL) using the original needles described below [4]. Still, the results were satisfactory, and many patients wished to undergo an operation. However, although the TVM procedure improved treatment outcomes enormously, complications during and after surgery have become a concern [5]. Complications during surgery include perforation of other organs such as the urinary bladder when the needle is manipulated, and postoperative complications include mesh exposure (erosion), pelvic and bladder pain, infection, pain during sexual intercourse with/without partner pain and urinary and other problems [6].
To suppress postoperative complications caused by mesh placement, it is desirable to reduce the area of the mesh used as much as possible without weakening the force supporting the vagina and uterus when the mesh is placed. Generally, the most important areas for vaginal and uterine support are assumed to be the upper part of the vagina and the cervix. Therefore, we devised an operative method that reduces the mesh area used to 56% that of the commercially available mesh pattern by eliminating the arms for the obturator muscle or foramen while supporting the upper part of the vagina and the cervix with the mesh.
In the present study, we evaluated the results and safety of our operative method that uses a reduced mesh size and also examined the factors related to postoperative POP recurrence by comparing the relapsed patients with the non-relapsed patients.
Go to : 
MATERIALS AND METHODS
1. Patients
This is retrospective study. The indication of operation were symptoms of vaginal prolapse, POP quantification (POP-Q) stage II or more and pessary treatment was unsuccessful. Between July 2014 and August 2015, 224 female patients underwent POP surgery. Exclusion criteria were a previous history of mid-urethral sling (MUS) procedure, recurrent cases after any operation for POP and other procedure of TVM. Ninety-one patients underwent the minimal mesh TVM operation.
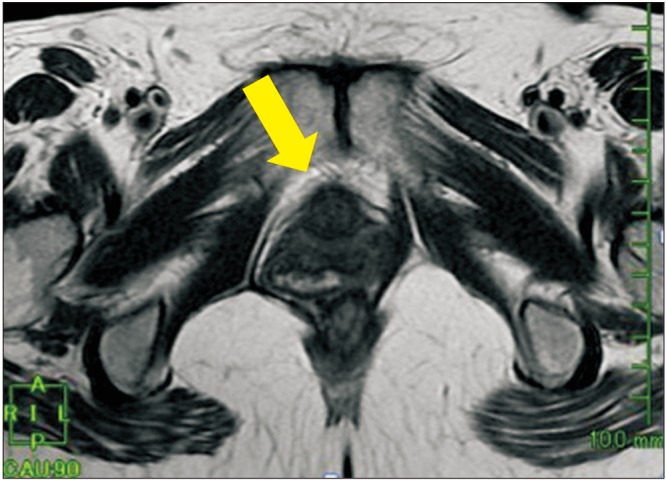
Age, body mass index (BMI), and parity were recorded. For lower urinary tract symptoms, the overactive bladder symptom score (OABSS) was assessed for daytime frequency, nighttime frequency, urgency, and urgency incontinence. Patient quality of life (QOL) was also assessed for general health, prolapse impact, role limitations, physical limitations, social limitations, personal relationships, emotions, sleep, and severity measures by the prolapse quality of life questionnaire (P-QOL), in which scores range from 0 (best health perception) to 100 (worst health perception). Avulsion defined as pubovisceral muscle detachment from the pubic bone on axial magnetic resonance imaging (MRI) was also assessed (Fig. 1). The degree of prolapse was evaluated in all patients by the POP-Q. Postoperative hospitalization was 2 days.
2. Surgical procedure
We performed operation by 3 surgeons. The surgical procedure was carried out under general anesthesia. As shown in Fig. 2, Polyform™ (15×20 cm; Boston Scientific, Natick, MA, USA) was cut in the shape of a 5×7-cm semicircle with 2 arms (Fig. 2A). First, hydrodissection was performed using 20 mL each of saline containing 1:1,000,000 epinephrine. The procedure was performed by making a midline full-thickness vaginal incision from the bladder neck to the uterine cervix and perforating the paravaginal space bilaterally. Both paravaginal and paravesical spaces were gently developed until the ischial spine and SSL were easily palpated. A skin incision was made 3 cm lateral to and 3 cm down from the anal verge (Fig. 2B). From this incision, we used a Shimada needle (Fig. 2C) with a hole on the tip threaded with nylon monofilament suture to penetrate the SSL, targeting two fingerbreadths (approximately 3 cm) medial to the ischial spine. Then, the mesh arms were placed using the nylon monofilament loops (Fig. 2D, E). The mesh was spread and fixed. Finally, traction over the exteriorized arms ensured correct positioning. In cases of a concomitant MUS procedure, it was performed through a separate incision.
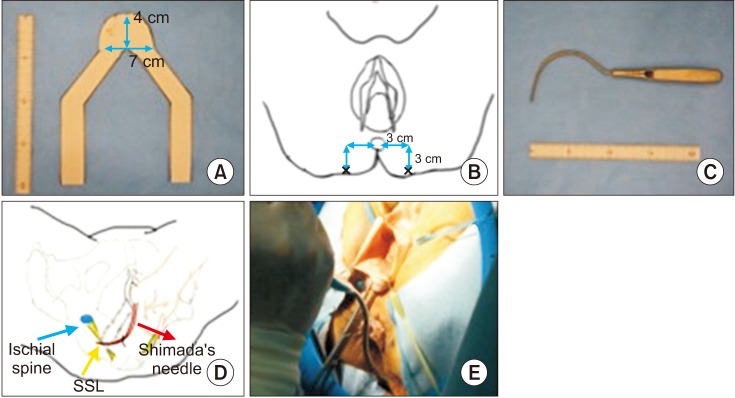 | Fig. 2Surgical details. (A) Polyform™ (15×20 cm, Boston Scientific, USA) is cut in a 5×7-cm semicircular shape with 2 arms. (B) The puncture point by the Shimada needle is 3 cm down on a vertical line from a point 3 cm lateral to the anal verge. (C) The original Shimada needle developed in Japan. (D, E) The needle and mesh arms pass through the location of the sacrospinous ligament (SSL) at a point that is 2 fingerbreadths (approximately 3 cm) medial to the ischial spine.
|
3. Methods
To assess the efficacy of our procedure, all patients underwent pelvic examination in the lithotomy position using the POP-Q system before and at one-year after the surgery. Objective recurrence was defined as the most dependent portion being at POP-Q stage II or more, which means that the most distal portion of prolapse is −1 cm or more from the plane of the hymen.
OABSS and P-QOL were evaluated before and at one-year after the surgery. We also assessed adverse events such as other organ injury, infection, mesh erosion, dyspareunia, and pelvic pain. Furthermore, de novo stress urinary incontinence (SUI) was evaluated in the patients in whom MUS was not performed at the time of the minimal mesh TVM operation.
Afterwards, to clarify the factors influencing the efficacy of our procedure, we compared several patient characteristics between the non-recurrence group and the recurrence group.
This clinical study was approved from the ethical committee of Yotsuya Medical Cube for publication (approval number: YCR16012).
4. Statistical analysis
Statistical analyses were performed with JMP ver. 11 (SAS Institute, Cary, NC, USA). Comparison of patient background between patients with and without recurrence was performed by the Mann-Whitney U test and chi-square test as appropriate. The Wilcoxon signed-rank test was used to analyze the OABSS and P-QOL scores before and at one year after the operation. A difference was considered statistically significant when p-value was <0.05.
Go to :
RESULTS
The characteristics of the 91 patients are summarized in Table 1. The mean age and BMI were 67 years (range, 48–83 years) and 22.8 kg/m2 (range, 17.7–33.2 kg/m2). Parity was 0 in one of 91 patients (1.1%), 1 in 13 patients (14.3%), 2 in 57 patients (62.6%), and more than 2 in 20 patients (22.0%). The median OABSS was 4.0 (range, 2.0–6.0). Avulsion was present in 24 of the 91 patients (26.4%). Regarding POP severity, 71 of the 91 patients (78.0%) were classified by the POP-Q system as stage III and 20 patients (22.0%) were stage IV. Thirty-five patients (38.5%) had past history of using pessary.
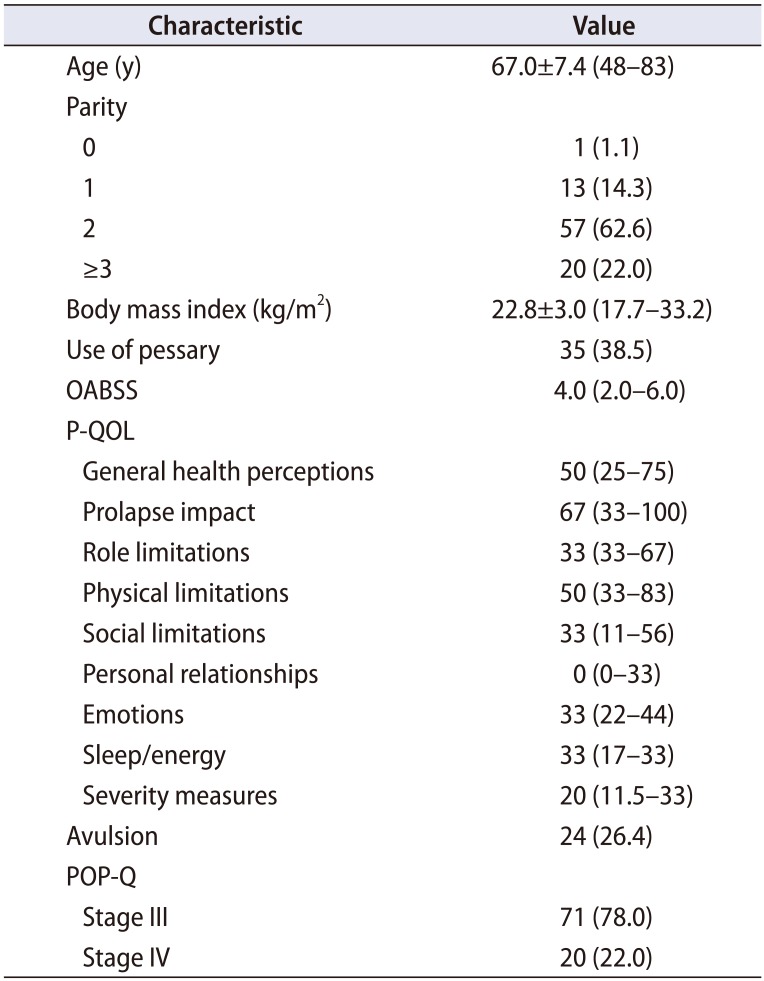
Table 1
Patient background (n=91)
![]()
Prolapse recurred in 10 of the 91 patients (11.0%), and all 10 were classified as stage II by the POP-Q system. The locations of recurrence in these 10 patients were POP-Q point Aa >−1 in 8 patients and Ba >−1 in 2 patients. However, no patients required additional surgical treatment for POP because they had no subjective symptoms. Thirty-seven of the 91 patients (40.7%) had OAB symptom before surgery. The OABSS improved significantly from 4.0 (2.0–6.0) to 2.0 (1.0–3.0) (p<0.01). There was significant decrease of symptom score in urinary frequency (p<0.01), urgency (p<0.01), and urgency urinary incontinence (p<0.01, Table 2). Eight of the 37 OAB patients (21.6%) remain the OAB symptom and postoperative de novo OAB was apparent in 3 patients (5.6%). Significant improvements were also observed for eight domains of the P-QOL (Table 2). The perioperative complication was pelvic hematoma and needed transfusion on postoperative day 1 (Clavien-Dindo classification II). This case didn't have massive bleeding during the surgery (TVM+tension-free vaginal tape [TVT]) and postoperative hospitalization was 3 days in this patient. No other major adverse events, i.e., the injury of other organs such as the bladder, urethra, and rectum occurred in our patients. Postsurgical complications were: mesh erosion that could be healed by focal treatment using vaginal estrogen tablets occurred in 2 of the 91 patients (2.2%) and pelvic pain in only one of the 91 patients (1.1%), whereas no infections and dyspareunia occurred. Regarding SUI, at the time of the minimal mesh TVM operation, a MUS was required in 48 of the 91 patients (52.7%). Furthermore, among the remaining 43 patients (47.3%), postoperative de novo SUI was apparent in 9 patients. Finally, additional surgery for SUI was performed in 2 of the 9 patients. Two of the 91 patients (2.2%) needed the catheterization for post-void residual urine. One of them underwent concomitant MUS procedure and required a tape cut surgical management under local anesthesia (Clavien-Dindo classification IIIa).
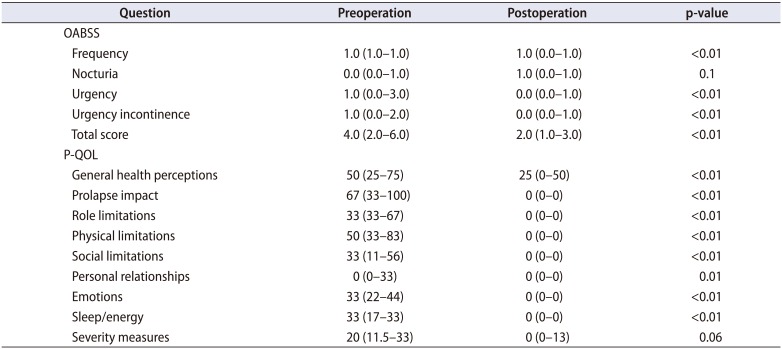
Table 2
OABSS and P-QOL score of before and one-year after the surgery (n=91)
![]()
To clarify the factors influencing the efficacy of our procedure, preoperative patient backgrounds were compared between patients with and without recurrence (Table 3). Although the age and parity number did not differ significantly, the BMI of the patients with recurrence (25.3±3.6 kg/m2) was significantly higher than that of those without recurrence (23.0±3.0 kg/m2, p=0.03). No significant difference was found in the OABSS. The rate of patients with avulsion was similar between the groups (27.2% vs. 20.0%, p=0.6). There were no significant differences in preoperative POP-Q point Aa (anterior vaginal wall 3 cm proximal to the hymen), Ba (most distal position of the remaining upper anterior vaginal wall), and C (most distal edge of the cervix or vaginal cuff scar).
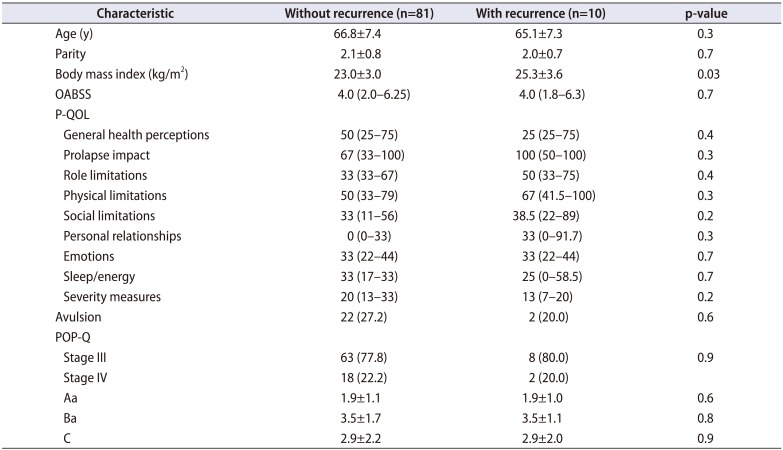
Table 3
Backgrounds of patients with and without recurrence (n=91)
Values are presented as mean±standard deviation, median (interquartile range), or number (%).
OABSS, overactive bladder symptom score; P-QOL, prolapse quality of life questionnaire; POP-Q, pelvic organ prolapse quantification; Aa, anterior vaginal wall 3 cm proximal to the hymen; Ba, most distal position of the remaining upper anterior vaginal wall; C, most distal edge of cervix or vaginal cuff scar.
Comparison of the rate of avulsion and POP-Q stage was performed by chi-square test and others were performed by Mann-Whitney U test.
![]()
Go to :
DISCUSSION
In this retrospective study, we found that our minimal mesh TVM procedure significantly improved anatomical outcomes in patients with severe prolapse at one year after surgery. Indeed, prolapse recurred in only 10 of the 91 patients (11.0%), all of whom were diagnosed as POP-Q stage II. Furthermore, most prolapses recurred at the POP-Q point Aa, and we did not experience any C >−1 recurrences. Previously, several studies showed an anatomic cure rate of 89% to 93% within 1 year after surgery (Table 4) [2789101112]. Recently, it was reported that the anatomic cure rate of patients with POP-Q stage <I was 94% at one year after surgery in procedures using the Uphold™ (Boston Scientific) [13]. The anatomic cure rate in the present study was 89.1%, which is as high as that reported in the previous studies, even though the mesh size in our procedure is 56% smaller than the original mesh design. Our minimal mesh TVM procedure has the great advantage of providing support for level I because the mesh arms in our procedure pass through the SSL, which is a pivotal ligament for supporting the vaginal edge. The SSL originates from the ischial spine and attaches to the lower part of the sacral bone and the lateral edge of the coccyx. The substantial support for level I offered by the connection with the SSL can cause adequate closure of the paravaginal space. Because the severity of prolapse of the anterior vaginal wall was reported to correlate with that of the vaginal edge, the support for level I is important to restore the damaged anterior vaginal wall [14]. Another study also reported that substantial support for level I is necessary for reinforcement of the anterior vaginal wall [15]. Our favorable results using a small mesh for large cystoceles and avulsion without the mesh arms passing through the obturator foramen may be explained by the strong tension in level I. Our procedure could also improve OAB symptoms (frequency, urgency, urgency incontinence) as evaluated by the OABSS. This is consistent with previous studies showing that frequency and urge incontinence as the representative symptoms of OAB were improved after vaginal hysterectomy with anterior-posterior colporrhaphy for POP [16]. But 21.6% patients remain the OAB symptom. It was reported that in patients with a higher preoperative PdetQmax do not showed improvement of symptom score in daytime frequency, urgency, urge incontinence or total OABSS score except nocturnal frequency [17]. We also found improvement in the P-QOL following our procedure. Although improvement of the scores for urinary-related symptom (urinary frequency, urgency, urge urinary incontinence, and SUI) in the P-QOL was already reported in a study with Japanese women [18], the present study showed that our procedure may be advantageous for QOL not only in terms of urinary-related symptoms but also for all 9 of the symptoms in the P-QOL.
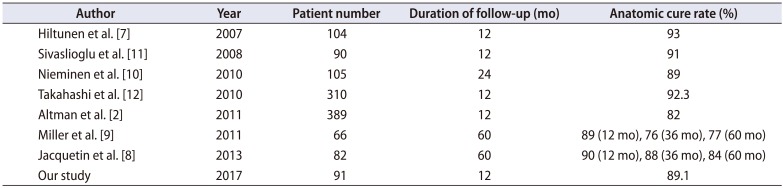
Table 4
Anatomic cure rate
| Author | Year | Patient number | Duration of follow-up (mo) | Anatomic cure rate (%) |
|---|---|---|---|---|
| Hiltunen et al. [7] | 2007 | 104 | 12 | 93 |
| Sivaslioglu et al. [11] | 2008 | 90 | 12 | 91 |
| Nieminen et al. [10] | 2010 | 105 | 24 | 89 |
| Takahashi et al. [12] | 2010 | 310 | 12 | 92.3 |
| Altman et al. [2] | 2011 | 389 | 12 | 82 |
| Miller et al. [9] | 2011 | 66 | 60 | 89 (12 mo), 76 (36 mo), 77 (60 mo) |
| Jacquetin et al. [8] | 2013 | 82 | 60 | 90 (12 mo), 88 (36 mo), 84 (60 mo) |
| Our study | 2017 | 91 | 12 | 89.1 |
![]()
Regarding adverse events, mesh erosion of the vaginal wall is the most common complication. Risk factors of mesh erosion are concurrent hysterectomy, T-shaped incision of the vaginal wall, age, smoking, and surgeons' experience [1920]. Especially, the lack of surgical experience resulting in creases, insufficient spreading, and insertion into the wrong layer of mesh can cause postoperative erosion. It was reported that mesh erosion occurs in 10.3% of patients on average, and 56% of them require surgical resection [19]. In the present study, we experienced only 2 patients (2.1%) with mesh erosion. Fortunately, both patients were asymptomatic and were managed using vaginal estrogen tablets. This low rate may be a result of our careful consideration of the appropriate location of mesh within the adventitia layer between the full thickness of the vaginal wall and the bladder. In addition, the reduction of mesh size in our procedure may help to prevent the formation of creases. Another important postoperative complication is dyspareunia. Rates of dyspareunia were reported to be as high as 8.9%. Mesh erosion and posterior colporrhaphy are considered to cause such pain [19]. None of the study patients complained of dyspareunia postoperatively, which may also be another benefit of the small mesh size. Although we found only one patient (1.1%) with pelvic pain, this patient's symptom improved gradually without intervention. In addition to the small size of our mesh, our modification to flexibly support the pelvic organs by penetration into the SSL without excessive tension may be associated with the circumvention of postoperative pain, especially that accompanying sexual intercourse. Another forte of our minimal mesh TVM procedure is its low rate of organ injuries. First, this method requires smaller areas of dissection. Second, our original Shimada needle facilitates penetration from the incision made beside the anus to the SSL. Shimada needle is curved about 90 degrees, it is easy to penetrate the SSL and catch the nylon monofilament suture. In fact, a one-fingerbreadth space is sufficient to allow for a safe penetration without any blind operation. These features of the minimal mesh TVM procedure appear to contribute to the reduced risk of organ injuries in the present study. Furthermore, we modified the approach to the SSL anteriorly in our procedure. Nevertheless, we usually approach the SSL posteriorly in a traditional TVM procedure. The safety of the anterior approach in bilateral SSLF was already reported [21]. That study pointed out that the SSL was well visualized and accessed through an anterior vaginal incision. Penetration of the SSL via the obturator foramen is risky because such a procedure carries a high risk of damaging the blood vessels surrounding the ischial spine. Instead, penetration to the SSL via the hip is conducive to circumventing such risks. We believe that our procedure is safe and ideal from the viewpoint of adverse events.
Several previous studies have been conducted to determine the factors influencing the recurrence of prolapse. One study reported that the severity of uterine prolapse and operators' experience were the independent factors [22], whereas other studies showed that avulsion detected by MRI and the kinds of mesh kits that pass through the obturator foramen were important factors [2324]. Unexpectedly, the preoperative POP-Q stage was not related to recurrence in the present study, and BMI was found to be the only factor influencing recurrence. BMI is generally well accepted to be an important factor in the outcome of the TVM procedure because obesity is closely associated with POP [25]. In addition, de novo SUI appeared postoperatively in 9 of the 43 patients without MUS (20.9%) at the time of the minimal mesh TVM procedure, although 2 of these 9 patients were forced to undergo an additional MUS procedure. Our rate of de novo SUI was similar to that of previous studies; 23.6% by Abbott et al. [26], and 37% by Kuribayashi et al. [27].
The strength of our study is that all patients were examined at female urology center and used validated questionnaires. The limitation is absence of a control group using commercially available kits or other way of TVM procedure. In addition, the lack of the analysis of some factors like smoking, medication, menopause, bladder function, which might have affected the results. Moreover, sexual activity rate was low, evaluation about sexual function might be not enough.
Go to :
CONCLUSIONS
Here, we report a favorable one-year outcome and low complication rates of our minimal mesh TVM procedure that does not use commercially available kits. After our operation, symptoms of OAB and QOL improved dramatically. Although a long-term, large-scale study will be necessary to evaluate our procedure, we believe that our procedure should be considered as one of the treatment options for POP.
Go to :
 XML Download
XML Download