

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Currently, shock wave lithotripsy (SWL) remains a widely accepted minimally invasive option for treating urinary stone disease [12]. Stones are first disintegrated by shock waves, and the fragmented stone particles are spontaneously cleared from the ureter and bladder [3]. Failed passage of stone fragments can obstruct the urinary tract, thus causing post-treatment complications such as flank pain, hydroureteronephrosis, and decreased renal function [45]. This failure can be caused by poor fragmentation efficiency so that large stone fragment obstructs the urinary tract. Alternatively, a particles of stones that are finely disintegrated can form an obstructing column of sand (Steinstrasse) in the ureter [6]. Steinstrasse formation following SWL is dependent on several factors, including stone burden, location and composition, and shockwave frequency and energy. Previous studies have shown that Steinstrasse following SWL occurs in 1%–4% of patients with small stones, 5%–10% of patients with large stone area (>2 cm2), and up to 40% of patients with partial or complete staghorn stones [7].
The increasing use of non-contrast computed tomography (NCCT) provides additional information including skin-to-stone distance (SSD) and attenuation value as mean Hounsfield units (HU) of stone [8]. Valuable information from NCCT may be a promising approach in predicting for Steinstrasse following SWL [9]. Nowadays, indications for SWL has been extended for large upper ureter calculi, thus even may cause post-SWL Steinstrasse formation [10]. Although predictive factors and clinical course of Steinstrasse following SWL for renal calculi have been described, little is known about such complication with ureter calculi. To address these issues, we investigated the predictive factors and clinical course of Steinstrasse formation following SWL for ureter stone
Go to : 
MATERIALS AND METHODS
Patient data were analyzed from November 2005 to May 2013 in 1,418 patients with one-session SWL at our medical institute. Patients had to fulfill the following inclusion criteria: 1) 4–20 mm sized single ureter stone; 2) radiopaque density on plain-film; 3) availability of pretreatment NCCT. Patients with multiple stones, single kidney, congenital urinary tract anomalies, or receipt of prophylactic medical expulsion therapy were excluded from analysis. Finally, 551 patients were enrolled in this retrospective study.
The detailed history and characteristics of patients with ureteral stones, including the number of history of stones, the time of onset of pain, and the characteristics of various characteristics were acquired. The characteristics of calculi included mean attenuation value (HU), SSD, location, and stone burden (maximal stone length and stone area). Attenuation value was measured by setting the bone windows in an axial NCCT scan image showing the maximum diameter of ureter stone [11]. The elliptical region was measured and the maximum area in stone was secured without containing the surrounding tissues as much as possible. The SSD was measured at 45 degrees in each vertical axis on axial image. The maximal stone length calculated by NCCT was the longest length in three dimensions including x-, y-, and z-axis of stone. We used commercially available picture archiving and communication system software for image analyses. Electroconductive lithotripter (Sonolith® Praktis; EDAP Technomed, Lyon, France) was used from 2005 to 2011 and electromagnetic generative lithotripter (Compact Delta II lithotripter; Dornier MedTech, Wessling, Germany) has been used since 2012 in our institute. A ureter stent insertion was considered prophylactically in patients with large stones (>15 mm) prior to SWL. All SWL were performed using fluoroscopic examination. The SWL was performed at 1–1.5 shock-wave per second between 2,500–4,000 shock-waves in a session with a focal peak pressure ranging from 16 to 55 MPa. When the stone identification became difficult during SWL or when the patient's degree of pain became unbearably severe, the session was terminated early. Treatment success was defined as complete clearance of the stones or presence of clinically insignificant residual fragments ≤3 mm without the need for auxiliary procedures within a 3-month follow-up period.
This study adheres to the Declaration of Helsinki and has complied with relevant laws and regulations and good clinical practice and ethical principles. Institutional Review Board of Severance Hospital approved the protocol of this study (approval number: 4-2014-1064). Because this study was a retrospective study, all participants' written informed consent was waived and all information was anonymized and preceded in a state where it could not be identified. The study quality was assessed by the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist.
Statistical analyses
Continuous variables are shown as the median and interquartile range. Differences in variables with continuous distributions were assessed using the Wilcoxon rank-sum test with continuity correction. Fisher's exact and χ2 tests were used to assess the difference between the categorical variables. Propensity score-matching with respect to patients' demographic factors and stone characteristics was employed to minimize selection bias. Non-Steinstrasse cases were 2:1 matched with the closest propensity with each Steinstrasse case [10]. Multivariate logistic regression analysis and Bayesian logistic regression model were performed to identify the predictors of Steinstrasse development following SWL for ureter stone. Detailed Bayesian statistical analysis method was described previously [1213]. All statistical analyses were performed using R software ver. 3.0.3 (R Foundation for Statistical Computing, Vienna, Austria), and the package ‘MatchIt’ and the package ‘Zelig and MCMCpack’ were used for propensity score-matching and Bayesian analysis, respectively.
Go to :
RESULTS
Table 1 shows the baseline characteristics of 551 patients who underwent single-session SWL for single ureteral stones. The incidence of Steinstrasse in ureter stone patients after SWL was 2.2% (n=12). The Steinstrasse incidence was significantly associated with stone size, attenuation value, and SSD in the comparison of the Steinstrasse group and the control group based on the NCCT characteristics of patients and stones. Steinstrasse patients had significantly higher stone sizes (stone size and stone area, p=0.005 and 0.003), higher stone attenuation (p=0.004), shorter SSD (p=0.009). Prophylactic ureter stenting was not a statistically significant predictor of Steinstrasse formation (p=0.231). After non-Steinstrasse cases were 2:1 propensity-matched with each Steinstrasse case, the Steinstrasse group had a significantly shorter SSD compared to the non-Steinstrasse group (p=0.013) (Table 2).
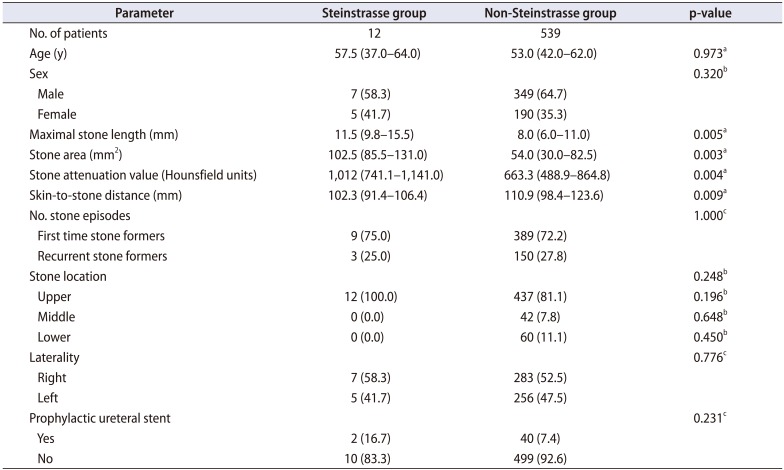
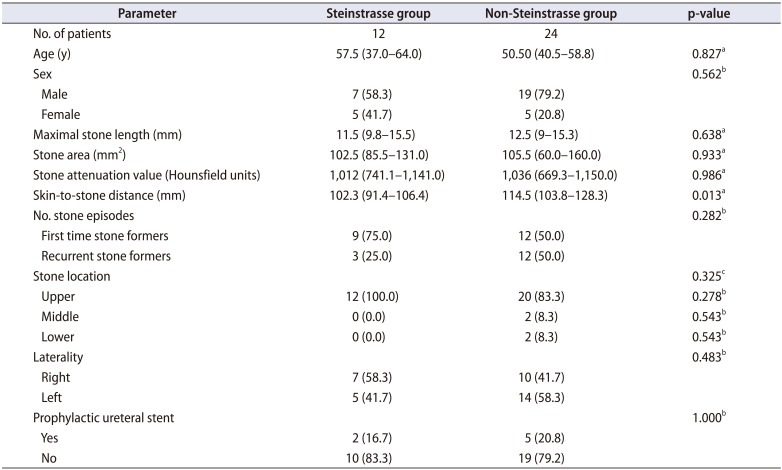
Table 1
Demographic data comparisons between Steinstrasse and non-Steinstrasse groups (n=551)
![]()
Table 2
Demographic data between Steinstrasse and non-Steinstrasse groups from matched cohort
![]()
The univariate logistic regression models for predictive factors of Steinstrasse following SWL for ureter stones revealed that stone size (odds ratio [OR], 1.160; 95% confidence interval [CI], 1.051 to 1.270; p=0.002), HU (OR, 1.003; 95% CI, 1.001 to 1.004; p=0.003), and SSD (OR, 0.968; 95% CI, 0.941 to 0.996; p=0.025) were significantly correlated with Steinstrasse formation (Table 3). In multivariate analysis, all stone NCCT parameters were independent predictors of Steinstrasse formation after SWL as a treatment for ureteral stones (Table 3). In the posterior distribution of the Bayesian logistic regression model, larger stone size (mean, 0.141; 95% CI, 0.018 to 0.253), higher HU (mean, 0.002; 95% CI, 0.001 to 0.005) and shorter SSD (mean, −0.024; 95% CI, −0.056 to −0.001) after SWL for ureter stones were important predictors of Steinstrasse development (Table 4). In Table 5, logistic regression model showed that maximal stone length and stone attenuation were significant factor for success following SWL, whereas SSD was not significant factor.
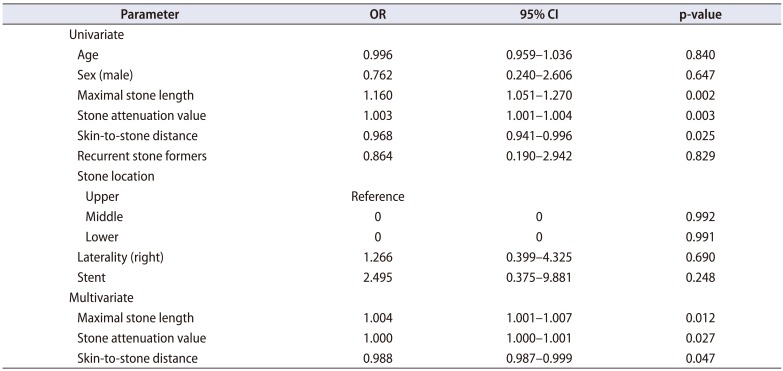

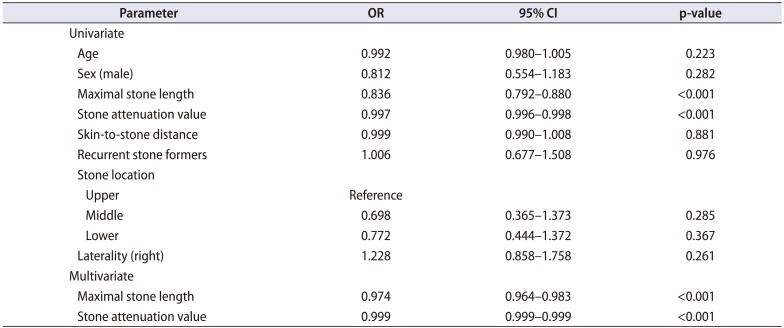
Table 3
Univariate and multivariate logistic regression models for predictive factors of Steinstrasse following shock wave lithotripsy for ureter stones
![]()
Table 4
Posterior distribution for Bayesian logistic regression models for predictive factors of Steinstrasse following shock wave lithotripsy for ureter stones
![]()
Table 5
Univariate and multivariate logistic regression models for predictive factors of success rate following shock wave lithotripsy for ureter stones
![]()
Of the 12 Steinstrasse patients, six received conservative treatment, and additional SWL was performed on the remaining six patients. In patients with repeat SWL, the average number of session of SWL was 2.83, and no serious complications occurred, such as acute pyelonephritis, urinary sepsis, or severe colic that necessitated an emergency room visit. None of Steinstrasse case needed cystoscopic ureteral stent insertion, percutaneous drainage, or consequent surgical intervention.
Go to :
DISCUSSION
Present study investigated the incidence and clinical significance of Steinstrasse after SWL for single ureteral calculi. The overall incidence of Steinstrasse after SWL for single ureteral calculi was relatively rare. Computed tomography characteristics of stones were significant predictors of Steinstrasse formation. If a patient has a high probability of Steinstrasse formation following SWL for ureteral calculi, appropriate patient counseling and consideration of ureteroscopic stone surgery is indicated.
Numerous predisposing factors are involved in Steinstrasse formation, including patient characteristics (i.e., age, renal morphology, and stone history), stone traits (i.e., stone number, size, composition and location), and lithotripsy related factors (i.e., shock wave frequency and energy level) [61415]. Madbouly et al. [6] reported that stone size and location, renal morphology, and lithotripsy energy are significant predictors of Steinstrasse development. Another study by Onal et al. [16] also supported that stone burden is a significant predictor for developing Steinstrasse in pediatric urolithiasis after SWL. Our results are similar to findings of previous studies, insofar as stone burden is a significant predictor for Steinstrasse development after SWL; however, the present study has important distinctions from previous studies. The important distinction of our study was that we considered additional diverse stone characteristics elucidated by NCCT. Although CT scanning has become recognized as a useful initial evaluation tool for assessing stone disease and provides valuable stone characteristics, no report has before evaluated these stone parameters as potential predictive factors for Steinstrasse development after SWL. HU and SSD evaluated by NCCT have been suggested as potential predictors of SWL success in patients with stone disease [317]. Previous clinical studies have suggested that greater stone attenuation is associated with SWL failure, which means high-density stones requiring more shock waves for fragmentation. SSD was considered a significant factor in approximately half of published related studies [18]. Pareek et al. [19] suggested that SSD, as a manifestation of obesity, outweighed body mass index as an independent predictor of SWL success. However, in an Asian population, Choi et al. [20] reported that SSD was not a significant predictor of SWL success in both patients with small (≤10 mm) or large (>10 mm) stones. Another study by Tanaka et al. [21] also demonstrated that there was no statistical difference in SSD between groups that experienced successful and failed SWL, and SSD was not a significant predictor for success after SWL. In this study, SSD was a significant predictor of Steinstrasse development following SWL, whereas not a significant factor for SWL success. One notable characteristic of the ureter stones was that they had a longer SSD than renal stones. From a study by Wiesenthal et al. [18], mean SSDs were 98.1±24.6 mm in renal stones and 130.1±25.7 mm in ureter stones, indicating that the SSD of ureter stones was approximately 3 cm longer than that of renal stones. Thus, SSD in ureter stones cannot be a significant predictor for successful outcomes following SWL. However, in ureter stones with relatively short SSDs, the effectiveness of shock waves can be determined in the early phase of SWL. At that time, a relatively large fragmented stone may migrate into the lower ureter by peristaltic movement of ureter, which can induce inappropriate stone focusing and patient positioning in the late phase of SWL.
A Steinstrasse is commonly transient, asymptomatic, and safely treated by conservative management [16]. Steinstrasse may initially be treated conservatively, but when there is obstruction, infection, or no stone fragment progression, another treatment should be considered, including repeated SWL, percutaneous nephrostomy, endoscopic intervention, and finally open surgery [22]. In large renal stones, Steinstrasse occurs in up to 40% of patients, and percutaneous or surgical intervention is necessary. On the other hand, all of our Steinstrasse cases were successfully managed by expectancy or repeat SWL monotherapy. None of our Steinstrasse patients develop serious complications such as acute pyelonephritic attack, urinary sepsis, or severe colic that necessitated an emergency room visit. None of our Steinstrasse cases also needed decompression of the corresponding renoureteral system or consequent surgical intervention. The smaller stone burden of ureter stones may be responsible for these favorable clinical outcomes.
Our study had some inherent limitations. Its retrospective design and small sample size may have introduced sampling bias. For example, prophylactic ureteral stenting was more preferred in patients with a large stone burden. Thus, we could not confirm the influence of prophylactic stenting on Steinstrasse development after SWL for ureter stones. Moreover, two different shock-wave generating machines may be a bias, but there was no statistical difference in each period. Finally, we did not categorize patients according to Steinstrasse type and extent because most affected patients had type I and short extent (1–2 cm). Despite these limitations, we applied a Bayesian modelling approach to overcome the retrospective nature and small sample size. We are confident in our novel findings regarding the clinical utility of discrete NCCT-derived stone parameters as predictive factors of Steinstrasse development after patients undergo SWL for ureteral stones. To our knowledge, this is the first study designed to describe and evaluate Steinstrasse after SWL for ureteral calculi.
Go to :
CONCLUSIONS
The incidence of Steinstrasse after SWL in ureteral stone patients was relatively rare and could be conservatively managed. Stone size, attenuation value and SSD were significant predictors of Steinstrasse development after SWL for ureter stone. Our result may provide important information that can be used to guide the treatment plan and counseling of patients with a high possibility of developing Steinstrasse after SWL for ureteral calculi.
Go to :
 XML Download
XML Download