

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Underactive bladder (UAB) has yet to be formally defined by any international academic society, such as the International Continence Society (ICS). Recently, an international expert group has described UAB as a symptom complex suggestive of detrusor underactivity (DU) that is usually characterized by prolonged urination time with or without a sensation of incomplete bladder emptying, usually with hesitancy, reduced sensation on filling, and slow stream [1]. Moreover, given Andersson's proposal to characterize UAB based on symptoms, a better term may be UAB syndrome, in analogy to the overactive bladder syndrome defined by the ICS [2]. Unlike UAB, DU has already been defined by the ICS as a contraction of reduced strength and/or duration resulting in prolonged or incomplete emptying of the bladder [3]. DU, which is urodynamically diagnosed based on a pressure-flow study, is characterized by a low-pressure, poorly sustained, or wavelike detrusor contraction associated with poor flow rate [4]. Considering its definition, UAB may have certain vagueness, given that the symptoms to be included in the syndrome still need to be discussed.
The lower urinary tract (LUT), including the urinary bladder and urethral sphincter, is regulated by simple circuits (on-off switching) that maintain an interactive relationship between the urinary bladder and the urethral outlet through which sufficient storage and voiding can be achieved. These reflexes are coordinated through complex neural interactions among the central nervous system (CNS) including pons, periaqueductal gray, brain frontal cortex, lumbosacral spinal cord, and peripheral nerves system (pelvic, hypogastric, and pudendal nerves), and storage and voiding reflexes are primarily organized in the spinal cord and the brain, respectively [5]. Sufficient urine output requires complete relaxation of the internal (smooth muscle) and external urethral sphincter (striated muscle), followed by increased intravesical pressure due to detrusor smooth muscle contraction [6]. It is highly probable that UAB is caused by one or several dysfunction(s) in the site (central and/or peripheral) innervating the micturition reflex.
CAUSES OF UNDERACTIVE BLADDER
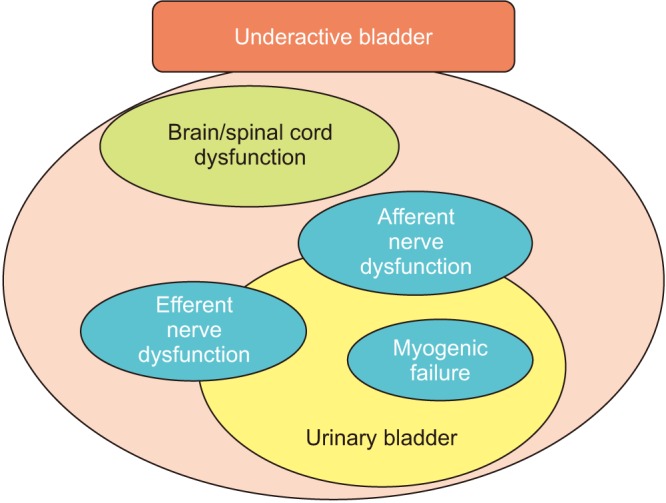
So far, several causes (diseases/disorders) of UAB have been reported [78]: aging [910], persistent bladder outlet obstruction (BOO) [11], diabetes mellitus (DM) [1213], neurologic disorders [14] (e.g., Parkinson disease, multiple sclerosis, and infectious neurologic problems, such as AIDS and herpes zoster), and nervous injury to the spinal cord, cauda equine, and peripheral nerves [1516] (e.g., spinal stenosis, pelvic fractures, and pelvic surgery). These cause impaired bladder function, especially voiding, and consequently result in DU/UAB, which undoubtedly deteriorates the patient's quality of life. To optimize treatment, we need to consider how such causes (diseases) contribute to impaired voiding function. Considering pathophysiological backgrounds, several contributing factors, such as intrinsic detrusor dysfunction (myogenic failure), efferent and/or afferent nerve dysfunctions, and dysfunctions in CNS control, have been reported (Fig. 1).
FACTORS CONTRIBUTING TO UNDERACTIVE BLADDER
1. Myogenic failure
Human detrusor smooth muscle bundles are arranged in a complicated pattern and surrounded by connective tissue containing significant amounts of collagen. From a functional viewpoint, however, the detrusor expands an integrated unit of interconnected muscle bundles [17]. The different bundles converge in the bladder neck, continue to the urethra, and then run an oblique or longitudinal course in the urethral wall. The muscles fade out distally in the connective tissues surrounding the urethral meatus. Impairment in the contractility of the detrusor smooth muscle, which can be attributed to “myogenic failure,” would directly lead to DU/UAB.
One of the major causes of myogenic failure is “aging.” Symptoms of urinary retention, urinary hesitancy, and incontinence, which are frequently observed with aging, have been attributed to UAB [181920]. Gilpin et al. [21] reported on age-related morphological changes, especially decreased axonal content of the human detrusor smooth muscle. Another histological examination that utilized human tissues demonstrated an increase in collagen deposition with aging [22]. In patients with UAB, similar histological changes, such as widespread degeneration of the axon, muscle loss, and fibrosis of the detrusor smooth muscle, were observed [23]. Moreover, Mansfield et al. [24] reported that mRNA expression of M3 muscarinic receptor decreased with aging and these changes may diminish the potential sensitivity of micromotional activity to cholinergic neurotransmitters. These age-related changes were recently confirmed and reported by Ito et al. [2526]. They demonstrated that aged rats showed weaker contractile responses to carbachol and electrical field stimulation related to decreased cholinergic-mediated contraction, lower M3 muscarinic receptor mRNA expression, and higher collagen deposition in isolated detrusor strips, and that cystometric investigations of aged rats showed greater postvoid residual volume and lower voiding efficiency. Pathophysiological changes in muscarinic receptors, especially the M3 muscarinic receptor subtype, and fibrosis can be theoretically and reliably considered as key factors for UAB.
2. Efferent nerve (motor nerve) dysfunction
Voluntary control of the LUT requires nervous interactions between autonomic (sympathetic and parasympathetic nerves) and somatic (pudendal nerves) afferent and efferent pathways [5]. In several pathophysiological conditions of LUT dysfunction [2728293031], deterioration of bladder efferent function may be due to peripheral denervation. Various factors, such as nerve damage (e.g., DM) [3233], ischemic/oxidative conditions (e.g., BOO and atherosclerosis) [343536373839], and oxidative stress [40], have been assumed to induce peripheral denervation.
Several studies have indicated that the isolated bladder itself shows autonomous micromotions (microcontractions), which increase with bladder distension, generate sensory (afferent) nerve activity, and become altered in cases of LUT dysfunctions [41424344]. During the voiding phase in a normal bladder, excitation of the parasympathetic efferent nerve causes the smooth muscles to contract synchronously, thereby increasing intravesical pressure. However, individuals with bladder efferent function deterioration, especially by denervation, would have an attenuated initial contractile force in the denervated areas. Therefore, these denervated areas might be able to contract only when there is excited propagation from a neighboring intact innervated area or via interstitial cells that are also present between the bundles of detrusor smooth muscle. Moreover, during voiding, the potential for micromotional propagation to recruit contraction in denervated areas may allow compensation for some loss of innervation. However, over time, extensive denervation may take too long to generate a rise in tone and contraction, which would lead to prolonged voiding durations with insufficient urine evacuation. Thus, the increasing severity of denervation would be associated with an attenuation of contractibility, causing impaired detrusor contractility [45]. Such processes have been suggested at least in aged mice [46].
3. Afferent nerve dysfunction
Throughout the bladder filling (storage) phase, the parasympathetic efferent innervation (pelvic nerve) to the detrusor is inhibited, whereas that to the urethral smooth and striated muscles (hypogastric and pudendal nerves) is activated, preventing urinary incontinence [47]. Bladder distention has been supposed to evoke afferent activity via myelinated Aδ-fibers connected in series with smooth muscle fibers [4849]. This in turn activates sympathetic outflow, (mainly via the hypogastric nerve), to the bladder outlet (the bladder neck and the urethra) and the pudendal outflow to the external urethral sphincter during the storage phase. Normal bladder distension activates low-threshold mechanoreceptive afferents coupled in series with detrusor muscle cells (myogenic pathway). However, unmyelinated C-fibers running in the suburothelial layer and even in the urothelium, coupled with urothelial cells and suburothelial interstitial cells, lead to signal transductions from the urothelium (urothelial pathway) [50]. Not only is the urothelium a barrier for harmful substances in the urine, it is also functionally active in the storage phase of micturition cycles [51]. In particular, the urothelium actively contributes to sensory functions, expressing various receptors for neurotransmitters [52], while urothelial cells are able to release neurotransmitters and signaling molecules, including nitric oxide, adenosine triphosphate, ACh, prostaglandins, substance P, and nerve growth factor [5354555657]. Urothelial cell-released substances may act directly on afferent nerves or indirectly via an action on suburothelial myofibroblasts (also referred to as “interstitial cells”) that lie near afferent nerves. Myofibroblasts are extensively linked to each other, as well as to afferent nerve fibers and detrusor smooth muscles, by gap junctions (electrical synapse) and can release substances that in turn act on afferent nerves [5]. Thus, urothelial cells and myofibroblasts are believed to contribute to sensory mechanisms in the urinary bladder by chemical coupling to the adjacent sensory nerves. Therefore, it is conceivable that age- or disease-related changes in the structure and function of the urothelium and afferent nerves could directly alter bladder afferent function.
Smith et al. [58] performed urodynamic studies in patients with LUT symptoms and found that those with DU may have defective volume sensation rather than impaired detrusor contractility, suggesting that reduced central sensitivity to volume sensation (i.e., mechanosensitive afferent activity) contributes to DU in nonobstructed, nonneurogenic symptomatic patients. Such observations are consistent with their previous reports wherein they show that peripheral and/or central sensory mechanisms may be important contributors to aging-related bladder dysfunction [959]. In addition, Azadzoi et al. [37] showed degenerating and collapsed axons, Schwann cells surrounded by dense connective tissue, and splitting of the myelin sheaths in a chronically ischemic bladder. Dahlin et al. [60] reported that thinly myelinated fibers were more susceptible to oxygen deprivation under ischemic conditions than thicker ones, whereas unmyelinated fibers were resistant to ischemic induction. Furthermore, attenuation of urothelial sensitivity to modulators of potassium channel activity has been observed in diabetic bladders [61], which may cause afferent sensory dysfunction [33626364], as well as contribute to contractile force and spontaneous activity of the detrusor smooth muscle [61]. Mohammed et al. [6566] reported that aged rats showed significant decreases in the expression of calcitonin gene-related peptide (CGRP) and substance P on the lumbosacral dorsal root ganglion neurons and in the density of pituitary adenylate cyclase-activating polypeptide innervation on the subepithelial plexus and the muscle layer of the bladder, whereas CGRP and substance P innervation on the muscle layer were slightly reduced. Moreover, Jiang and Kuo [67] recently reported that patients with DU had a significantly lower expression of E-cadherin, which plays an important role in cell adhesion. They additionally demonstrated a decrease in the expression of M2 and M3 muscarinic receptors, P2X3 purinergic receptors, and endothelial nitric oxide synthase and an increase in the expression of β3-adrenoceptors in patients with DU [67]. These findings clearly show that directly altered sensory transduction and impaired urothelial signaling pathways appear to be the pathophysiological conditions for UAB/DU.
4. Brain/spinal cord dysfunctions
Symptoms of incomplete bladder emptying, which has been attributed to UAB, are also commonly observed in patients with specific neurological diseases: multiple sclerosis [68], Parkinson disease [69], and multiple system atrophy [70]. The common pathologic findings in multiple sclerosis are focal demyelination and plaque formation throughout the CNS (brain to spinal cord), which delay and/or block nervous system communication (nervous conduction), including sensory afferent function [71]. Regarding the relationship between lesion sites and symptoms, a previous study demonstrated that patients with cervical cord or pontine lesions were more likely to suffer from UAB/DU, whereas those with cerebral cortex lesions were more prone to having storage symptoms, and detrusor overactivity (DO) [72]. Although the underlying pathophysiology of UAB/DU in Parkinson disease is still unclear, it is conceivable to correlate UAB/DU with the patient's overall motor function in the brain areas, including the frontal cortex, basal ganglia, thalamus, anterior cingulate gyrus, and caudate nucleus. Moreover, Kim et al. [73] recently reported that patients with multiple system atrophy had higher incidences of DU compared to those with Parkinson disease, although the pathophysiology of UAB/DU still remains uncertain.
Almost all patients with spinal cord injury (SCI) initially show UAB/DU or acontractile detrusor during spinal shock, which subsequently develop into chronic bladder dysfunctions depending on the level of spinal cord lesions. For patients with supra-lumbosacral SCI, the parasympathetic and sensory spinal centers in the sacral spinal cord are preserved; however, synaptic reorganization leads to the appearance of involuntary bladder contractions during bladder filling, i.e., neurogenic DO [747576]. In addition, the coordination between bladder contractions and urethral sphincter relaxation guaranteed by the pontine, where well known as micturition center, becomes impaired. Instead, bladder and urethral sphincter contractions occur simultaneously, such phenomenon leading to an event known as detrusor-sphincter dyssynergia.
Injuries in the sacral spinal cord or cauda equina could lead to chronically persisting DU or acontractile detrusor. In an animal model of cauda equina lesions, Sekido et al. [77] reported on the pathophysiology of UAB induced by lumbar spinal canal stenosis (LCS). Two weeks after surgery in rats with LCS, cystometry results showed that postvoid residual urine volume and the number of nonvoiding contractions increased, whereas voided volume, threshold pressure, and maximum intravesical pressure decreased. Moreover, isolated bladder strips showed an increase in the contractile response to electrical field stimulation. Interestingly, they reported no obvious changes in the detrusor muscle's contractile response to carbachol stimulation and its morphology in LCS rats.
ANIMAL MODELS FOR UNDERACTIVE BLADDER
Due to ethical concerns, direct experimentation on human subjects with UAB has been limited, requiring studies to utilize animal models of UAB as an alternative. Ideal animal models are those that mimic part of human pathophysiology and/or a functional problem. Thus far, several animal models mimicking clinical UAB, which show “prolonged urination time” and/or “reduced contractile strength,” have been reported, especially in rodents.
1. Diabetes mellitus
In an animal model related to DM, streptozocin-injected animals (rodents) have been widely used [323378]. This DM model is relatively guaranteed the experimental reproducibility with higher glucose blood level, but simultaneously needs to pay attention to the differentiation from the influence of polyuria, which can be distinguished by sucrose-induced polyuria animal model [63]. Moreover, genetical DM animals have long been used and recognized as mild DM model, which may be similar to type II DM in human [7980818283].
3. BOO
Surgery for the creation of BOO is basically similar among several studies, but the degree of obstruction sometimes depends on the techniques, animal species, and sexes [87]. Although a short period of time of obstruction shows sign of UAB [8889], prolonged periods of obstruction (chronic or persistent BOO) generally appears as more severe UAB [34899091].
4. Nerve injury (especially of the pelvic nerve)
There have been several published studies reported as a UAB model by using pelvic nerve crash- or cryoinjury (unilaterally or bilaterally) [9293949596], in which detrusor contractility was remarkably impaired. In case of bilateral pelvic nerve injury by complete resection, the animals showed severe nervous dysfunctions, which were resemble to the situation with SCI [95].
5. Ischemia
Ischemic models have long been investigated on bladder dysfunctions [60979899]. To address more clinical situation, atherosclerosis models have recently been reported [37100], and the animal with longer period of time of atherosclerosis may be a better candidate as an ideal UAB model [3839].
Given the absence of alternative tools for determining the pathophysiology of UAB, an animal model needs to be used. However, species differences between animals and humans should be considered. Moreover, an appropriate animal model of UAB has not been established, because UAB carries multifactorial symptoms and has yet to be properly def ined. To advance pathophysiological understanding and develop medical interventions including pharmacotherapy for UAB, various animal models need to be further established.
CONCLUSIONS
The pathophysiology of UAB/DU includes failure in detrusor muscle contractility, bladder efferent and afferent nerve dysfunction, and failure of the CNS to coordinate voiding function. Though a few publications have helped us better understand the complex pathophysiological mechanisms of UAB, many uncertainties still remain, particularly in the role of aging, altered sensory function, and the translational value of existing animal models.
 XML Download
XML Download