

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Prostate cancer (PCa) is the second most common cancer, with nearly 1,000,000 cases diagnosed per year and the third most common cause of cancer-related deaths in men worldwide [1]. Radical prostatectomy (RP) is a largely successful method of treatment for PCa [2]. The presence of prostate-specific antigen (PSA) in the circulation immediately after RP indicates a failure to eliminate the PCa completely, and the reappearance of PSA at a later stage indicates a PCa relapse [2]. About one-third of men may develop biochemical recurrence (BCR), which is defined as an increase in PSA levels after treatment with RP or external beam radiation therapy (EBRT) [34]. PSA progression after RP of clinically localized PC is a common problem for both the patient and physician. Careful monitoring, EBRT, and androgen deprivation therapy could be the treatment options for these patients. However, treatment of increased PSA levels after RP is a complex and controversial issue.
In patients with benign prostatic hyperplasia, 5-alpha-reductase inhibitors (5-ARI) reduce PSA levels by 50% to 66% [5]. Recently, the role of dutasteride in PC has sparked some interest. Two prospective studies have shown that treatment with dutasteride reduces the risk of PC [67]. In addition, dutasteride delayed the BCR for clinically localized PC in Avodart After Radical Therapy for Prostate Cancer Study (ARTS) [89]. To date, however, there have been no studies that have investigated the effect of early dutasteride administration on PSA in men with detectable serum PSA following RP. In this study, we investigated the effect of early use of dutasteride on serum PSA levels in men with detectable serum PSA levels following RP.
MATERIALS AND METHODS
1. Ethics and informed consent
This study was conducted at Wonkwang University Hospital. Written informed consent was obtained from all subjects before enrollment in the study. Study protocols and informed consent forms were approved by Wonkwang University Hospital Institutional Review Board (WKUH 201603-HRE-30).
2. Study design and subjects
This study was a prospective, open-label study with a cumulative analysis of asymptomatic increase in PSA following RP in patients aged less than 85 years. Two hundred eighty-one RPs were conducted from January 2005 to December 2013. Follow-up was conducted until July 2015 for all patients. Patients underwent RP by one of the following techniques: retropubic RP, laparoscopic RP, or robot-assisted RP. Clinical and pathological data were collected. The clinical data included age at the time of RP, preoperative PSA level, postoperative PSA level, and prostate volume determined by transrectal ultrasound (TRUS). The TRUS-guided prostate biopsy was performed with 12 cores at peripheral zone. The pathological data included Gleason score for prostate biopsy, percent positive biopsy cores (the percentage of overall number of cores with cancer), pathological Gleason score, pathologic T stage, and positive surgical margins. TRUS-guided prostate biopsies were performed by urologists with an 18-gauge needle biopsy gun. An early PSA increase was defined as a detectable serum PSA level>0.04 ng/mL. The lowest serum PSA level in our institution was 0.04 ng/mL. Patients undergoing adjuvant EBRT or androgen deprivation therapy were excluded from the study. Patients with a PSA level of >0.04 ng/mL were treated with dutasteride 0.5 mg daily as soon as it was detected during follow-up. The serum PSA level was checked every 3 months and BCR were monitored. BCR was defined as a PSA level of 0.2 ng/mL following RP, which was confirmed by at least 2 consecutive measurements. We divided the patients into 2 groups according to the serum PSA response after dutasteride treatment. PSA response was defined as a serum PSA decrease of greater than 10% after treatment with dutasteride.
3. Statistical analysis
The clinicopathological data were compared between the 2 groups: patients who showed PSA response after dutasteride treatment and those who did not. Continuous variables were compared using the 2-sample t-test, and categorical variables were compared using the chi-square test. Univariate and multivariate logistic regression analyses were performed to determine the predictive factors for PSA response. The results were considered significant at a p-value of <0.05. All statistical analyses were performed using SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
A total of 80 patients were included in the study. Baseline characteristics are provided in Table 1. The mean age of the patients who received RP was 67.6 years (range, 47–77 years). Twenty-one patients (26.3%) received retropubic RP, 15 received laparoscopic RP (18.8%), and 44 received robot-assisted laparoscopic RP. At the median follow-up period of 51.8 months, 56 patients (70.0%) showed a serum PSA level decrease of greater than 10%, and 24 showed increased PSA levels. All the patients with increased PSA levels showed BCR. After BCR, patients received androgen deprivation therapy or radiotherapy. Twelve of the 56 patients with a PSA response showed subsequently increased PSA levels.
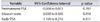
Preoperative PSA levels (p=0.028), PSA nadir levels (p=0.030), and Gleason score of 6 or less (p=0.035) were significantly different between the PSA responder group and PSA nonresponder group in univariate analysis (Table 2). A multivariate analysis revealed that a Gleason score of 6 or less (p=0.018) and PSA nadir levels (p=0.011) were predictive factors for PSA response after early treatment of dutasteride in men with a increased PSA following RP (Table 3).
DISCUSSION
The major finding of our study is that early monotherapy with dutasteride showed a decrease in serum PSA levels in men with detectable serum PSA after RP. Dutasteride may delay BCR after RP. The rationale for the routine use of dutasteride after radical therapy in PC patients is currently under debate. However, as dihydrotestosterone (DHT) is the most potent androgen in the prostate, inhibition of 5-alpha-reductase isoenzymes, which convert testosterone to DHT, could be an appropriate target for the treatment of PCa [10]. Moreover, 5-ARIs monotherapy that can prevent PCa with minimal complications could be a good therapeutic option in men who have undergone RP.
Andriole et al. [11] showed that treatment with dutasteride resulted in almost complete suppression of intraprostatic DHT, increased apoptosis, and decreased microvessel density. These findings suggest that dutasteride can cause regression in PCa. Iczkowski et al. [12] reported that after short-term dutasteride treatment, benign epithelium showed involution and epithelial shrinkage, and PCa tissue demonstrated a decrease in epithelium relative to stroma. These findings indicate that dutasteride induces significant phenotypic alterations in both benign and neoplastic prostate, supportive of a chemopreventive role or chemoactivity. However, these studies were conducted in subjects who did not receive radical therapy for PCa. Perrotti et al. [13] reported the results of treatment with dutasteride in BCR patients. In a prospective, single institution study of dutasteride monotherapy following RP, 46% of men experienced a serum PSA decrease of more than 10%, and 25% had a serum PSA decrease of more than 50%. PSA doubling time (12 months) and a Gleason score (6 vs. ≥7) were associated with a better response to dutasteride, but only PSA doubling time was statistically significant. The authors suggested that dutasteride monotherapy delayed or prevented the progression of PCa in men with BCR after RP [13]. ARTS showed the clinical significance of dutasteride on BCR in patients with PCa [89]. Treatment with dutasteride for 24 months significantly delayed the PSA doubling time compared with the placebo group. Relative risk reduction was 66.1% (95% confidence interval, 50.35–76.90) for the overall study period. Dutasteride significantly delayed BCR compared with the placebo group [9]. There were some differences in our study design compared with previous studies. Patients with detectable serum PSA (0.04 ng/mL) following RP, but not after BCR, were treated with dutasteride 0.5 mg daily. These findings can provide potential evidence for dutasteride treatment for the prevention of PCa after radical therapy.
Andriol et al. [14] evaluated the effect of finasteride in patients who underwent RP. They reported that finasteride showed a delayed increase in serum PSA compared with a placebo of approximately 9 months in the first year and 14 months by the end of the second year. However, these differences were not statistically significant. The reduction in local and distant recurrences in the finasteride group suggests that the effect on PSA reflects a direct effect on tumor growth without affecting the initial response to subsequent hormonal therapy.
No single factor can be considered definitive towards the prediction of BCR. Preoperative PSA, clinical stage, Gleason score after RP, tumor volume, perineural invasion, and vascular invasion are the most important clinical and pathological parameters for assessing detectable PSA after RP [15]. Results of our study showed that preoperative PSA, nadir PSA (p=0.030), and biopsy Gleason score 6 or less (p=0.035) after RP were significantly different between PSA responder group and PSA nonresponder group. A multivariate analysis that revealed a Gleason score 6 or less and nadir PSA were predictive factors for PSA response after early treatment of dutasteride in men with a rising PSA following RP. These findings could give information on the expectation of response to dutasteride treatment after radical therapy in PC patients.
Our study, however, has some limitations. This was a single-arm study, and the results of this study cannot be compared with the results of those who did not take dutasteride. Moreover, this study was a single institutional study, which did not include a large population. A large and randomized prospective study is required to confirm these findings. To date, the adverse side effects of 5-ARIs on sexual function have received minimal attention and were deemed clinically less important [16]. However, in patients who have undergone RP, these sexual side effects could be an important issue. Another potential concern is that 5-ARI treatment for PCa may shorten the time for development of resistance to androgen deprivation therapy, despite 5-ARIs being the subject of long-term follow-up (7 years) clinical trials and in clinical use for more than 10 years [17]. However, 5-ARI may have utility as less aggressive treatment options for patients who have rising PSA after RP, and in patients with PSA progression having resistance to androgen deprivation therapy.
CONCLUSIONS
In this study, early monotherapy of dutasteride showed a decline in serum PSA levels in men with lower nadir PSA levels, and a Gleason score 6, when the serum PSA was detected after RP. Dutasteride may delay BCR after RP in low risk PC. However, a large and randomized prospective study is required to confirm these findings.


 XML Download
XML Download