

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Urolithiasis is one of the most common disorders of the urinary tract and affects approximately 5% to 10% of the population. There has been a progressive increase in prevalence in recent decades that has reached close to 20% in economically developed countries [12]. This increase is similarly proportional for cases of ureterolithiasis, where a higher morbidity and mortality of lithiasic pathology is reflected in high costs for the health system (approximately 2 billion United States dollars annually in the United States) [1].
Because ureterolithiasis is a high-incidence pathology, the complications are equally frequent [3]. The objective of current treatment is to resolve the ureteral obstruction with minimal complications. Many descriptive studies have reported spontaneous expulsion rates of up to 50% for all calculi and up to 85% for calculi <5 mm in size between 28 and 40 days [45]. When spontaneous expulsion does not occur, it is possible to use minimally invasive therapeutic modalities, which are highly effective but not innocuous procedures that are responsible for a large part of the cost overrun for the health system. Thus, the therapeutic spectrum has shifted towards improving medical expulsive therapy (MET) by seeking more accurate indications and more effective medications to reduce the complications associated with both the surgical intervention and the circumstance of inappropriately postponing it.
Selective alpha-blockers, such as tamsulosin and silodosin, and calcium antagonists, such as nifedipine, have traditionally been the treatment of choice, with proven efficacy in multiple clinical trials. Additionally, in the last decade, the possibility of using phosphodiesterase type 5 inhibitors (PDE5i) in MET has been studied owing to their direct effects on the relaxation of the ureteral smooth muscle in both animal and human models. This effect impacts the frequency of the peristaltic waves and the muscle tone of the ureter along its entire extent. Vardenafil appears to play a leading role in the in vitro models, followed by sildenafil and tadalafil, with potent effects on the formation of the derived second messengers cyclic guanosine monophosphate and cyclic adenosine monophosphate [6]. However, the independent mechanisms of action of nitric oxide formation have been questioned because this pathway alone accounts for between 20% and 30% of the detected effect. Some authors have suggested that the inhibition caused by the influence of ionic calcium by 2 routes would intervene in ureteral smooth muscle contractions [67]. Owing to the aforementioned considerations, the possibility of studying the efficacy of PDE5i in the MET of patients with distal ureterolithiasis has been proposed.
The objective of this review was to determine the efficacy of PDE5i as monotherapy in MET of distal ureteral calculi of less than 10 mm.
MATERIALS AND METHODS
This study was conducted according to the recommendations of the Cochrane Collaboration following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. The protocol was registered in the international prospective register of systematic reviews (PROSPERO; https://www.crd.york.ac.uk/PROSPERO/) under number CDR42016038858.
1. Selection criteria
1) Studies
Parallel randomized clinical trials performed between January 1980 and May 2016 were included. Open and closed trials and studies with simultaneous interventions were excluded. No language restriction was imposed.
2) Participants
Women and men over 18 years of age who were diagnosed with single, unilateral symptomatic distal ureterolithiasis with a ureteral calculus of 10 mm or less in its largest dimension were included. Studies that included patients with acute renal injury secondary to the ureteral obstruction, monorenal patients, or patients with associated urinary sepsis, bilateral or multiple ureterolithiasis, or concomitant treatment with PDE5i were excluded.
2. Information sources and search strategy
A search strategy was designed for controlled clinical trials published in MEDLINE (National Library of Medicine, Bethesda, MD, USA) via the Ovid (Wolters Kluwer, New York, NY, USA), CENTRAL (Cochrane Library, London, UK), and Embase (Elsevier, Amsterdam, The Netherlands) databases. The search strategy was specific for each database and included a combination of medical headings and free text terms for ureteral calculi and types of studies. A specific search was performed with indexed terms and free writing for sources of conference abstracts, clinical trials in progress (www.clinicaltrials.gov), literature published in nonindexed journals, and other sources of gray literature. A generic search strategy was designed for Google Scholar (Google Inc, Mountain View, CA, USA). No language restrictions or publication statuses of the articles were considered. Articles were included from January 1980 to May 31, 2016. The complete search strategy for each database is listed in Supplementary material.
3. Study selection
Two investigators reviewed the titles and abstracts independently and blinded to determine the potential usefulness of the articles within the systematic review. The eligibility criteria were applied during the review of the full text of potentially eligible articles for the final selection. Discrepancies were resolved by consensus of the 2 researchers.
4. Data collection process
Relevant data were collected in duplicate by using a standardized data extraction sheet that contained the study design, participants, interventions and comparators, and final outcome details. The reviewers confirmed all data entries and checked for completeness and accuracy at least twice. If some information was missing, we contacted the authors to obtain complete data.
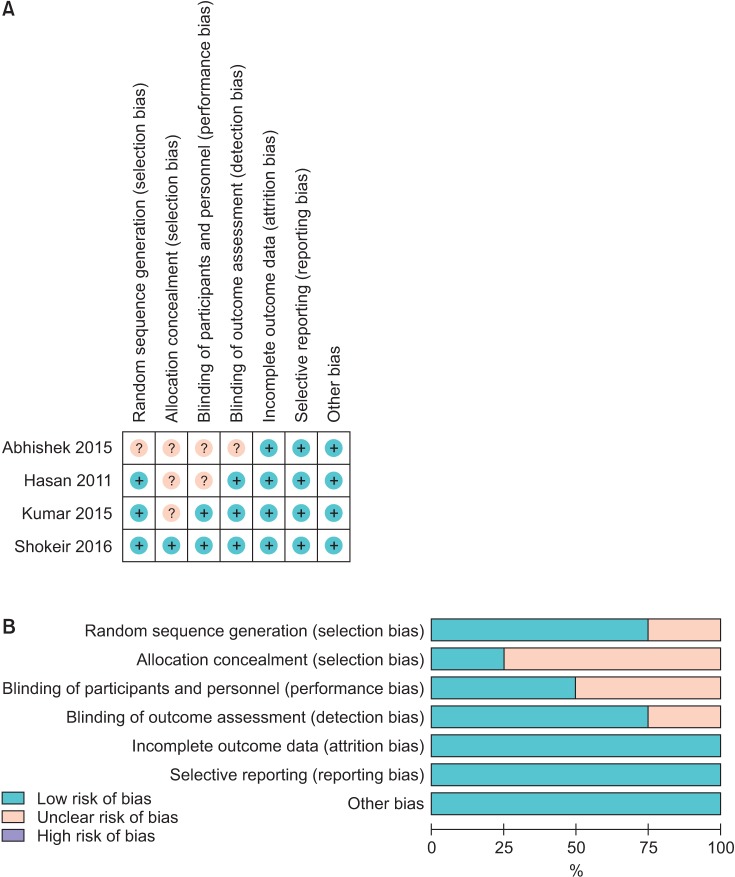
Risk of bias in and across individual studies was assessed independently by 2 researchers using the Cochrane Collaboration risk of bias tool. We solved disagreements by consensus.
The “Risk of bias table” was edited by using Review Manager Software ver. 5.3 (RevMan; Cochrane Collaboration, Copenhagen, Denmark) to illustrate the judgments for each study. A risk of bias summary was made to show the judgments in a cross-tabulation of study by entry.
5. Summary measures
Analyses were performed in RevMan 5.3 and Stata 13 (StataCorp., College Station, TX, USA) as needed. The risk ratio and the risk difference (RD) were the effects measured for the primary and secondary outcomes with 95% confidence intervals (95% CIs). We performed a randomeffects meta-analysis to assess heterogeneity (clinical and statistical) in the included clinical trials.
Heterogeneity between trials was assessed through the I2 statistic. An I2 value greater than or equal to 50% could represent heterogeneity according to Higgins et al. [8]. The results were reported as forest plots showing the effect size of all included studies with 95% CIs.
6. Additional analyses
No meta-regression was performed owing to the number of included studies. We undertook the sensitivity analysis based on the exclusion of each one of the trials, but no differences were found [9]. Analysis of publication bias was not performed owing to the number of studies found (less than 10 studies) according to Higgins et al. [8].
RESULTS
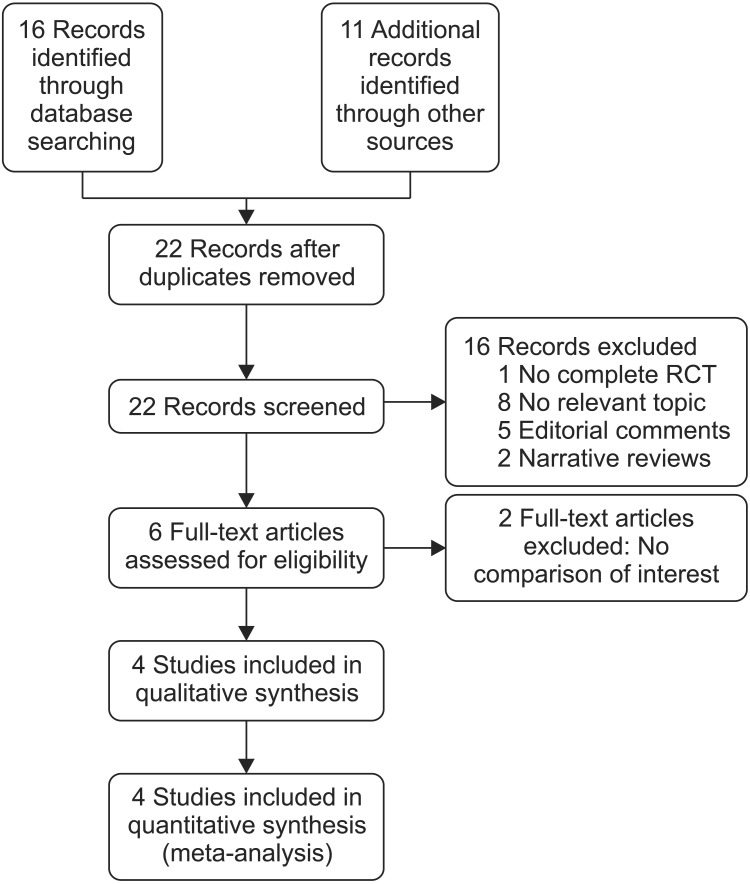
Study selection: A total of 27 records were found with the search design strategies. Among them was a phase III clinical trial in progress that had recently completed the recruitment period and thus had no results available. Finally, four studies were included in the qualitative and quantitative analysis (Fig. 1) [10111213].
Characteristics of the included studies: The selected studies included 580 patients with a median of 145 patients per study (range, 60–270). The 4 studies evaluated the calculus expulsion rate at 28 days as a primary outcome [10111213]. All studies reported the time to expulsion as one of the secondary outcomes and provided information regarding the response to pain and the side effects during treatment, with the exception of the study by Abhishek et al. [12]. Three studies used comparisons with a placebo [101112], 1 study used sildenafil [10], and 3 studies used tadalafil as the PDE5i (Table 1) [111213].
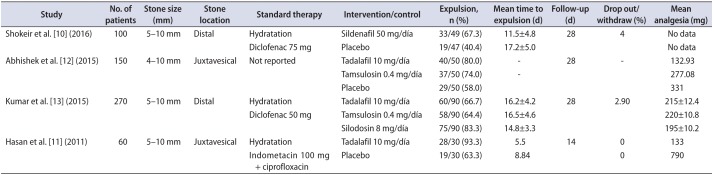
Table 1
Characteristics of the included studies
| Study | No. of patients | Stone size (mm) | Stone location | Standard therapy | Intervention/control | Expulsion, n (%) | Mean time to expulsion (d) | Follow-up (d) | Drop out/withdraw (%) | Mean analgesia (mg) |
|---|---|---|---|---|---|---|---|---|---|---|
| Shokeir et al. [10] (2016) | 100 | 5–10 mm | Distal | Hydratation | Sildenafil 50 mg/día | 33/49 (67.3) | 11.5±4.8 | 28 | 4 | No data |
| Diclofenac 75 mg | Placebo | 19/47 (40.4) | 17.2±5.0 | No data | ||||||
| Abhishek et al. [12] (2015) | 150 | 4–10 mm | Juxtavesical | Not reported | Tadalafil 10 mg/día | 40/50 (80.0) | - | 28 | - | 132.93 |
| Tamsulosin 0.4 mg/día | 37/50 (74.0) | - | 277.08 | |||||||
| Placebo | 29/50 (58.0) | 331 | ||||||||
| Kumar et al. [13] (2015) | 270 | 5–10 mm | Distal | Hydratation | Tadalafil 10 mg/día | 60/90 (66.7) | 16.2±4.2 | 28 | 2.90 | 215±12.4 |
| Diclofenac 50 mg | Tamsulosin 0.4 mg/día | 58/90 (64.4) | 16.5±4.6 | 220±10.8 | ||||||
| Silodosin 8 mg/día | 75/90 (83.3) | 14.8±3.3 | 195±10.2 | |||||||
| Hasan et al. [11] (2011) | 60 | 5–10 mm | Juxtavesical | Hydratation | Tadalafil 10 mg/día | 28/30 (93.3) | 5.5 | 14 | 0 | 133 |
| Indometacin 100 mg + ciprofloxacin | Placebo | 19/30 (63.3) | 8.84 | 0 | 790 |
![]()
Characteristics of the excluded studies: The reasons for exclusion were indications other than MET for the distal calculi, no clinical trials, interventions in combination with other medications, duplicates, and no relationship to the topic (Fig. 1).
Risk of bias in the studies: An evaluation of the risk of bias for the expulsion rate and the time to expulsion was performed owing to their close relationship in the evaluation of these outcomes; thus, the same information was required for their presentation. Kumar et al. [13] and Shokeir et al. [10] showed a low risk for the majority of the items, whereas Abhishek et al. [12] showed no clear risk for the first 4 evaluation items and a low risk for the rest (Fig. 2).
1. PDE5i vs. placebo: results according to the outcome
1) Expulsion rate of the ureteral calculus
Three studies [101112] included 256 participants (129 in the PDE5i group and 127 in the placebo group). According to our analysis, no heterogeneity among the studies was found; therefore, a fixed effects model was used for the analysis. The PDE5i were associated with a significantly higher expulsion rate than the placebo (79% vs. 53% [RD, 0.26; 95% CI, 0.15 to 0.37]) (Fig. 3A).
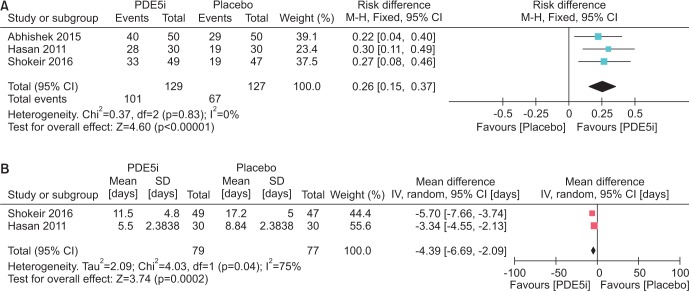
2) Time to expulsion
Two studies [1011] included 160 participants (80 in the PDE5i group and 80 in the placebo group). The PDE5i were associated with a significantly lower time to expulsion than the placebo (RD, -4.39; 95% CI, -6.69 to -2.09). Significant heterogeneity was found with an I2 index of 75%; therefore, a random effects model was used for the analysis of the data (Fig. 3B).
3) Use of analgesia
Two studies evaluated the use of analgesia during the course of the MET. However, the studies could not be included in the quantitative analysis because they differed widely in follow-up times and the analgesic used as the standard therapy. Abhishek et al. [12] described the use of minor oral diclofenac in the tadalafil group compared with a placebo during 28-day MET (132.93 mg vs. 331 mg, respectively, p<0.0001), whereas Hasan et al. [11] described the use of minor oral indomethacin in the tadalafil group compared with a placebo during 14-day MET (133 mg vs. 790 mg, respectively, p<0.0001). Similarly, both studies described a decrease in the number of ureteral colic episodes and a lower average pain score according to the visual analogue scale during MET.
4) Side effects associated with MET
Only one study described the side effects associated with treatment. Shokeir et al. [10] reported a frequency of uncomplicated cephalalgia of 4% in the intervention group and 0% in the placebo group in their study of sildenafil vs. placebo, although the difference was not significant (p=0.0579). Other effects of the treatment were not reported in this study.
2. Tadalafil vs. tamsulosin: results according to the outcome
1) Expulsion rate of the ureteral calculus
Two studies [1213] included 280 participants (140 in the tadalafil group and 140 in the tamsulosin group). According to our analysis, no heterogeneity was found among the studies; therefore, a fixed effects model was used. The efficacy of tadalafil was comparable with that of tamsulosin, with a nonsignificant risk difference of 4% in favor of tadalafil (RD, 0.04; 95% CI, -0.07 to 0.14) (Fig. 4).

2) Time to expulsion
Only one study reported time to expulsion as a secondary outcome. Kumar et al. [13] reported no significant differences when comparing tadalafil vs. tamsulosin in terms of time to expulsion of the calculus (16.2±4.2 vs. 16.5±4.6, respectively, p=0.648).
3) Use of analgesia
A single study reported the comparison between tadalafil and tamsulosin in terms of the use of analgesia. Kumar et al. [13] reported no significant differences when comparing tadalafil vs. tamsulosin, with an average use of diclofenac of 215±12.4 vs. 220±10.8, respectively (p=0.8).
4) Side effects associated with MET
Only one study described the side effects associated with treatment. Kumar et al. [13] reported multiple side effects associated with treatment, including cephalalgia, dizziness, back pain, orthostatic hypotension, and abnormal ejaculation. The frequencies varied between 3% and 15.5%, with cephalalgia (10%–15.5%) and dizziness (10%–15.5%) being more frequent. No significant differences were found for the frequency of each symptom mentioned when comparing tadalafil and tamsulosin (p≥0.05).
DISCUSSION
Ureteral colic is primarily due to ureterolithiasis, which represents approximately 1% to 2% of admissions to emergency services. The natural course of lithiasic disease must be balanced with the risks of surgical intervention. Therefore, MET has recently emerged as a therapeutic alternative for the initial treatment of distal ureterolithiasis in selected patients [14]. Some of the therapeutic approaches in MET include alpha-blockers, calcium antagonists, and corticosteroids. A decrease of peristalsis, reduction of inflammation, and relaxation of the ureteral smooth muscle are the basis for the use of these medications. However, the true indication for MET is confined to distal ureterolithiasis with a calculus diameter of between 5 and 10 mm. There is clear and consistent evidence of the high probability of expulsion of minor calculi up to 5 mm, which in some reports is close to 85% [45]. This issue has been a source of constant errors in the methodological designs of many studies that attempt to elucidate the efficacy of MET, because they include this group of participants in whom the probability of expulsion, per se, without intervention is quite high. Moreover, participants with calculi of the middle and even proximal ureter have been included, which contrarily may dilute the differences in favor of MET, leading to unexpected conclusions, as Pickard et al. stated in a more recent prospective study [1415].
Recently, the multiple mechanisms of action of PDE5i have increased the number of therapeutic indications for this pharmacological group. Taher et al. reported the presence of PDE1, 2, 4, and 5 isoenzymes in cytosolic solutions of human ureteral tissue, which suggested nonadrenergic ureteral motility mechanisms and even mechanisms independent of nitric oxide [1617]. Based on the same principle and on the in vitro effects on ureteral smooth muscle [67], PDE5i have been proposed as an option for MET.
This study is the first controlled systematic review and meta-analysis of clinical trials published to date. We attempted to determine the efficacy of PDE5i in MET. In summary, PDE5i are superior to placebos as MET, achieving a 26% increase in the probability of expulsion and decreasing the time to expulsion of the ureteral calculus by 4.3 days. The results of the latter outcome are subject to the presence of significant heterogeneity in the measurement of the effect (I2 index of 75%), which is principally explained by 2 factors: (1) 1 of the 2 studies included only calculi of the juxtavesical portion, which theoretically would reduce the time of expulsion and possibly the expulsion rate proportionally, and (2) the time of MET was 14 days instead of 28 days, which was in contrast to the majority of the studies on this topic.
Apparently, PDE5i could also improve the painful experiences of the patients during treatment by reducing the episodes of ureteral colic and the amount of analgesia required for their relief. However, there is insufficient information available to summarize the evidence in a quantitative analysis.
No differences were found for any of the outcomes evaluated in the comparisons of tadalafil vs. tamsulosin. This finding may be consistent with the pharmacodynamics of these 2 groups of medications and suggests the possibility of a synergistic combination that could increase the effectiveness of each of the drugs when administered separately. This hypothesis was proposed by Kumar et al. [18] and Jayant et al. [19] in 2 clinical trials, in which the expulsion rate for tadalafil plus tamsulosin ranged between 83% and 84%.
One of the strengths of our review was the quality of the search strategies designed for each database, which were highly sensitive and specific for the detection of records related to the question of the systematic review. Additionally, the characteristics of the included studies are highlighted because they included only patients with calculi between 5 and 10 mm, which is a group that has a real indication for MET as mentioned previously. Supporting these inclusion criteria, there is an ongoing randomized clinical trial from Mansoura University in Egypt (NCT02519153) comparing the efficacy of sildenafil versus placebo that has the same kind of participants in terms of calculi size, location, and following time. That trial supports the finding of this systematic review that MET was well-indicated in all included studies. The fact that new trials are focusing on this group of patients will add homogeneity to future updates of this topic.
The limitations of the systematic review and meta-analysis primarily included the small number of available studies and the quality of reporting of the clinical trials that composed them. This limitation does not necessarily indicate bad or good methodological quality. However, this variable could incur underestimation of the quality because the best tool available to evaluate quality is the Cochrane Collaboration tool, which requires an appropriate report to properly weigh the items. Nonetheless, the studies generally had a low risk of bias for the tool items.
Finally, this review was conducted to answer a question in relation to a highly prevalent urological pathology based on standardized recommendations. Therefore, although we recommend this intervention for various institutions worldwide, we suggest conducting trials with larger sample sizes and better methodological quality to improve the recommendations derived from this systematic review and meta-analysis.

 XML Download
XML Download