

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Urologic diseases are more prevalent in geriatric hospitals than in other hospitals. Dementia, stroke, cerebral infarction, and spinal disc herniation are common diagnoses in geriatric hospitals, and these conditions cause concomitant neurogenic bladder and other voiding difficulties [12]. In addition, most patients in geriatric hospitals have difficulty walking or are bedridden [3456], which also contributes to the prevalence of urologic diseases.
To manage urologic disease properly, a urologist must be involved. Indeed, one study showed that urologists are critical in improving urinary continence after bladder training [7]. Despite this, of the 3,326 medical specialists working in geriatric hospitals in December 2013, only 38 were urologists [8]. Such a paucity of urologists leads to poor management of voiding problems. In fact, according to previous research of South Korea, 84.4% of patients in geriatric hospitals received inadequate management for urinary incontinence [9]. Improper management of voiding disorders decreases quality of life and can even exacerbate existing conditions and comorbidities in the long term. The primary goal of geriatric hospitals is not to treat acute illness, but rather to manage chronic disorders and prevent the decline of daily function. To this end, it is essential that these hospitals manage voiding disorders properly.
Recently, no field studies have been carried out into urologic disease management in South Korean geriatric hospitals. Furthermore, given that the number of geriatric hospitals has risen exponentially, and that few such institutions employ an in-house urologist, voiding disorders in geriatric hospitals may not be well managed. On a different note, data from the National Health Insurance Service (NHIS) provide limited information, because they represent medical insurance data rather than the actual state of the field. For these reasons, we aimed to assess, using a field survey, the actual management status of urologic diseases in South Korean geriatric hospitals.
MATERIALS AND METHODS
1. Data acquisition
We analyzed 13 hospitals, of which 2 were in Seoul and 11 were in Incheon. We conducted patient surveys and in-depth interviews with medical personnel, between January 2014 to December 2014. The surveys and person-to-person interviews were all performed by urology specialists, fellows, residents, or nurses. Basic information regarding the hospitals and patients was gathered using a written questionnaire, and interviews with medical personnel were conducted in the same way (Supplementary materials 1,2,3). Importantly, we did not gather any information that identified the patients or medical staff. The person-to-person interviews were given by the patients themselves, except when they were unable to communicate; in such cases, the interviews were given by caregivers or nurses on the patients' behalf.
2. Ethics statement
This study was approved by the Institutional Review Board of Seoul National University Hospital (approval number: E-1410-080-618).
3. Statistical analysis
We used IBM SPSS Statistics ver. 19.0 (IBM Co., Armonk, NY, USA) for statistical analysis. The following additional information was also surveyed: the availability of urological consultation and outsourced medical care, as well as the number of (1) hospital beds, (2) staffed beds, (3) medical staff members, (4) geriatric care workers, and (5) physicians (numbered according to their medical specialties). The patient assessment included medical history, history of urological diagnoses, current urogenital problems, voiding symptoms, and urological intervention. In-depth interviews with medical personnel consisted of questions about the current management of urological disorders, as well as possible strategies for improvement.
RESULTS
1. Characteristics of participating geriatric hospitals
We included geriatric hospitals that were established between 2006 and 2014: 2 in Seoul and 11 in Incheon. Ten of the 13 institutions were certified geriatric hospitals; the mean hospital capacity was 215.2 beds (range, 110–367), with an average of 189.1 patients (range, 90–345) at the time of the study. Regarding healthcare staff, the hospitals had an average of 6.2 doctors (range, 3–11), and 40.2 nurses (range, 10–83). Of the 80 medical specialists across all institutes, there were no certified urologists. Only four of the hospitals (30.8%) provided routine urological consultation services, while 8 (61.5%) provided outsourced consultation on an as-needed basis (Table 1).
2. Patient Information
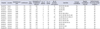
A total of 1,858 patients were enrolled in this study, among whom there were 358 (19.3%) in Seoul and 1,500 (80.7%) in the Incheon province. Nine hundred 2 patients (48.5%) were men, 955 (51.4%) were women, and 1 was of undetermined sex. The mean age was 69.6±15.1 years, and the average hospital stay was 10.0±9.1 months. The primary complaints upon admission were stroke (37%), dementia (26%), and gait disturbance (17%). There were also degenerative neurological disorders (8%), organic neurological disorders (6%), fractures (3%), pulmonary disease (2%), and neuropsychiatric disorders (1%). Common comorbidities were hypertension (62.0%), diabetes (49.4%), cardiac disorders (9.6%), spinal disorders (5.9%), and hepatic disorders (1.9%). Only 418 patients (22.5%) could walk unsupported; 515 (27.7%) required either a wheelchair or braces, and 252 (13.6%) required assistance from at least one person, and 644 (34.7%) were bedridden. On admission, 531 patients (28.6%) had at least one diagnosed urological disorder, such as urinary tract infection (UTI), benign prostatic hyperplasia, or neurogenic bladder.
3. Prevalence of urological disorders and treatment pattern
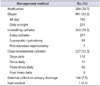
With regard to the prevalence of urological disorders, 900 patients (48.4%) had voiding difficulty, 930 (50.1%) had urinary incontinence, and 1,190 (64%) had both conditions. Almost half of incontinence patients (45.8%) suffered severe incontinence; requiring at least five pads per day. Three hundred eighty-four patients (20.7%) were on voiding disorder-related medications, and 1,109 patients (59.7%) were managed using a urinary intervention; namely diapers, indwelling catheters, clean intermittent catheters (CICs), or External collection urinary drainage (Table 2). Only 7% of patients were managed by urologist and 83% of patient had no medical advice for voiding problems (Fig. 1).
4. Frequency of complications
Urologic complications related to voiding difficulty were found in 375 patients (20.2%), and 350 patients (18.8%) had secondary complications related to urological disease. The total prevalence of urological complications was 39.0%, including duplicates (Table 3).
5. Medical personnel survey results
A total of 779 medical personnel participated in our survey, with a mean age of 40.1±8.5 years (range, 22–62 years). Most participants was female (90.4%) and 2 were of unknown sex. With regard to occupation, nurses (58.3%) and geriatric care givers (27.3%) were most common. About 43.5% of medical personnel recognized “over half” of patients in geriatric hospitals has urologic problem, but only 29.8% were planned routinely check-up by urologist. None of the patients received care from a certified urologist employed in the same hospital. Surprisingly, 0.9% of medical personnel replied that either the patient or their personal care giver were responsible for genitourinary care. Medical personnel reported that patient's genitourinary problems were relatively well managed. However, almost all of them agreed to needs of urologist (Table 4).
DISCUSSION
From 13 geriatric hospitals in the Seoul and Incheon areas, 1,858 patients and 779 medical caregivers participated in our survey. The reply rate among patients was 75.6% (1,858/2,458), while that among medical personnel was 77.5% (779/1,031). Considering many patients in geriatric hospitals either have difficulty communicating or co-operate poorly because of their coexisting medical condition, the present study was quite well encompassing. To increase response rate, we simplified questions and sometimes discuss with patient's family and care-giver. For example, we evaluated the prevalence of voiding disorders and incontinence using the following simple questions: “Have (you) experienced voiding difficulty or problems during the last 1 month?”, and “Have (you) experienced incontinence, regardless of self-will, during the last 1 month?”
We discovered several problems with the management of voiding dysfunctions in geriatric hospitals. Firstly, urinary incontinence was too often managed using urological interventions. Current literature recommend that geriatric patients be treated using behavior modification or bladder relaxant medication [21011]. Special undergarments such as diapers are only useful for patients with refractory incontinence [12]. In this study however, about a half of all admitted patients used a diaper to manage voiding problems. Secondly, the urologic interventions were not properly preformed. For instance, CICs can relieve urinary incontinence in the elderly, but they are inadequately used in geriatric hospitals. It is recommended that the CIC be used at a minimum of every 4 to 6 hours to minimize bacterial dwell time [13]; however, none of patients in the present study catheterized more than 3 times a day. Moreover, 16.2% of the patients performed inadequate external collection urinary drainage by tying a plastic bag around the penile glans, primarily to prevent diaper expenditure.
Furthermore, the incidence of complications was much higher in the present investigation than in other studies, which have reported a point prevalence of 1.5%–1.6% in longterm care facilities [1415]. In the current study, about onethird of patients experienced voiding problems related to complications, and 12.5% suffered from a UTI. Indeed, UTI is the most common bacterial infection in the elderly, and the risks of sepsis and septic shock are higher than in younger patients [16]. In addition, cognitive impairment increases UTI risk in the elderly [17], and vice versa [18]. For this reason especially, it is important that UTIs be managed properly in geriatric hospitals. The duration of urinary catheterization is a well-known risk factor for catheter-associated UTIs [19], and suprapubic catheterization prevents catheter-associated bacteremia more effectively. Despite this, 19.5% of inpatients are subjected to long-term indwelling catheterization, and most catheterized patients have an indwelling urethral catheter. On a different note, dermatitis is associated with improper management of diapers or external collection urinary drainage. Indeed, incontinence-associated dermatitis can be reduced by changing pads more often, as well as by using the proper pad type [20].
Relatedly, few urologists work in geriatric hospitals. According to the 2013 statistics of South Korea [21], only 1.6% of doctors working in geriatric hospitals were urologists, which is much lower than the average 7.5% among the eight major specialties. Indeed, gynecologists (4.5%) and practitioners of Korean medicine (6.8%) each comprised a much higher proportion. The present field study revealed that, among patients who required urological care, 83% did not receive treatment; moreover, fewer than 5% of urological disorders were diagnosed, and the diagnosis was always carried out by a nonurologist. Medical personnel agreed that more urologists were needed. Of the 779 medical personnel surveyed, 56.4% replied either “yes” or “highly required” when asked if they thought a urologist would benefit their patients. The diagnosis and management of UTIs and incontinence are complicated in the elderly population, and inadequate treatment increases patient mortality [22].
The simplest and most efficient solution to this would be to employ certified urologists in geriatric hospitals around the nation. Failing that, we believe that there are limits to a hospital's ability to outsource consultations, and that routine visits from an urologist provide a more realistic solution. In addition, including urological assessment criteria in current hospital accreditation systems, or in the Health Insurance Review and Assessment, may provide sufficient incentives to self-implement such systems. For example, The Korean Urological Association Insurance Committee suggested adding queries regarding “incontinence improvement rate,” “UTI incidence,” and “diaper usage” to the 2015 6th Korean National Health Insurance Value Incentive Program. Similarly, urological problems could be evaluated by including categories like “urinary catheterization rate,” “assessment of voiding function,” “Foley indwelling catheter rate,” and “consultation rate for urological problems”; such changes would likely improve healthcare. Furthermore, these criteria could standardize the quality of urological management in geriatric hospitals, and would probably be useful in establishing long-term medical policy.
Previously our group reported of 11 hospitals survey report within capital area [23], about knowledge and management pattern of urinary incontinence who work in geriatric hospitals. This study based on same cohort with additional 2 hospitals medical personnel and all 13 hospitals patients survey reports. The current study includes actual field data and provides insight into the current incidence of voiding disorders, as well as their management in geriatric hospitals. The data may inform medical policy decisions in future. The purpose of our study was to assess the current management of urological disorders in geriatric hospitals in South Korea, and to improve the quality of care for patients who are denied basic urological treatment. If geriatric hospitals continue improper management, the prevalence of complications will increase, leading to decreased quality of life and unnecessary suffering. More importantly, neglect of voiding disorders leads to poor hygiene, essentially stripping patients of their right to proper medical care.
Because field studies were limited to hospitals located in the Seoul-Incheon areas, our data may not accurately represent care in geriatric hospitals around the nation. On the other hand, even fewer medical specialists are employed in the provincial areas, and we therefore fear that management may be even worse there. Previous literature has shown that research based solely upon data requested from hospitals is limited, especially when assessing disease prevalence and patient management. Nonetheless, we believe that this study may provide useful reference data in the assessment of urological disorders throughout the nation.
CONCLUSIONS
Two-thirds of patients in geriatric hospitals suffer from urological problems and above half of these are undergoing a urological intervention; however, none of them are managed by a certified urologist. We believe that assigning more urologists will improve the management of urologic diseases in geriatric hospitals.




 XML Download
XML Download