

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chlamydia trachomatis (CT) is the most common cause of sexually transmitted infections (STIs) worldwide [1]. It is well established that in male patients CT can be one of the causes of lower urinary and male genital tract infections, with prostatitis-like symptoms and decreased fertility impairing male health [23]. CT has been accepted as a causative agent of chronic bacterial prostatitis (CBP), and for this reason testing for this pathogen is highly recommended [4]. Even if more than 50% of men with CT infections are asymptomatic, acute manifestation of the infection is responsible for a number of symptoms, infertility, and longterm reduced quality of life [56]. In addition, it has been demonstrated that CBP due to CT is an important organic cause of premature ejaculation, affecting the prostate ejaculation process [7]. Moreover, the treatment of prostate CT infection can be a real challenge for urologists, with the result being multiple recurrences and persistency of infection. The National Institutes of Health (NIH) classification of prostatitis includes all CBP, regardless of the causative agent, in class II [8]. Therefore, CBP due to CT is in the same category as that caused by common bacteria. It is unclear, however, whether there are any differences in the course or clinical outcome of the disease when the cause is CT or other uropathogens. In the present study, we aimed to evaluate the natural history, clinical characteristics, and outcome of CT infection compared with infection due to common uropathogens.
MATERIALS AND METHODS
1. Study design
All patients with clinical, microbiological, or instrumental diagnosis of CBP and attending the same STI clinic from January 2008 to December 2010 for prostatitis treatment and management were consecutively enrolled in this prospective parallel-cohort study. We chose this kind of study because in a prospective parallel-cohort study the groups of individuals (cohorts) are selected on the basis of certain factors and followed for a period of time to discover a possible relationship on defined outcomes [9].
2. Population
All enrolled patients were divided into 2 groups according to the microbiological findings: cohort A included patients with CBP resulting from CT infection, and cohort B included patients with CBP caused by common uropathogenic bacteria.
Assignment to each cohort was determined by molecular, immunologic, and culture results as follows. Cohort A included patients with positive results for CT DNA amplification in expressed prostatic secretions (EPS) and/or postprostatic massage urine (VB3) samples obtained from the Meares and Stamey test and negative results for common uropathogens. Cohort B included patients with negative results for CT DNA amplification and positive results for the following bacteria, considered as uropathogens: enteric gram-negative rods, enterococci, Staphylococcus saprophyticus, and group B streptococci [10].
3. Inclusion and exclusion criteria
Inclusion criteria for this study were a clinical and microbiological diagnosis of CBP (category II, NIH classification) and symptoms lasting more than 6 months. Diagnostic procedures for CBP were carried out in accordance with European Association of Urology guidelines [11]. Patients <18 and >45 years of age, with major concomitant diseases or anatomic abnormalities of the genital and urinary tracts were excluded. Moreover, patients with positive findings for CT infection in the first-voided urine specimen (VB1) or the midstream urine sample (VB2) of the Meares and Stamey test were excluded as well. Isolated positivity to serum anti-CT IgA and/or IgG was not considered a sufficient diagnostic criterion for CT infection, and therefore such patients were also excluded.
4. Microbiological considerations
All patients underwent a full microbiological diagnostic workup including cultures in order to detect common uropathogenic bacteria and yeasts, DNA extraction, and mucosal IgA evaluation for CT diagnosis and a Meares- Stamey four-glass test, performed according to the European Association of Urology guidelines [11]. Semen samples for culture were also collected and analyzed [11]. Genital samples were collected from each patient in accordance with indications described in a previous report: early-morning VB1, VB2, EPS, VB3, and seminal sample were sampled in sequence [12]. A culture of a urethral swab on each patient was performed to rule out urethritis as a result of CT infection [512]. The Meares-Stamey 4-glass test indicates the presence of bacterial prostatitis only if the bacterial load in the EPS or VB3 is at least 1,000 colony-forming units/mL and at least 10 times higher than in VB1 or VB2. Moreover, we considered a positive Meares-Stamey test result for every patient found with a significant number of bacteria in EPS and/or VB3. All samples were collected and immediately transferred to the laboratory, under refrigerated conditions, to be analyzed for cultures, DNA extraction, and polymerase chain reaction as described previously [512]. In accordance with Nickel et al. [13], the white blood cell count in all biological samples was obtained but not considered in this study. Each patient also underwent serum IgA and IgG anti-CT analysis. Blood sample collection was performed on arrival at the STI Centre [5]. Mucosal IgA was detected by a modified version of the IPAzyme Chlamydia IgG/IgA immunoperoxidase test (Savyon Diagnostics, Ashdod, Israel) [5]. We assigned a predefined score (i.e., from 1+ to 20+ points) in an attempt to quantitatively define the levels of mucosal IgA present in all samples, according to Mazzoli et al. [5]. The “plus” value of each score was dependent on the color intensity of intracellular inclusions caused by CT in infected fibroblasts, which was utilized as antigen in the analytical procedure and evaluated by microscopic reading (400 magnifications) [5]. Analysis of IgA in mucosal secretions analysis was performed by CT IgG + IgA Western blot (AID Autoimmun Diagnostika GmbH, Straberg, Germany). Blotted CT proteins were lipopolysaccharide (2 fractions), major outer membrane protein 1 (MOMP; 2 fractions), MOMP 2 (29, 45, 80 kD), HSP 60, and HSP 70.
5. Questionnaires and clinical examinations
The Italian versions of the following validated questionnaires were administered to each patient at the first visit and at each follow-up visit, as is routine practice in our center:
In accordance with Nickel et al. [19], prostatitis-like symptoms were considered significant at an NIH-CPSI pain score equal to or higher than 4.
6. Study schedule
Once enrolled, all patients were scheduled for annual follow-up visits at the end of the therapy, and in the presence of symptoms, until the end of the follow-up period. At each follow-up visit they were asked to complete the questionnaires and underwent clinical and microbiological examinations. All symptomatic recurrences were recorded and treated with antibiotics, depending on the organism, according to susceptibility testing, in line with the European Association of Urology guidelines [11]. In cohort B, all patients were treated in line with the antibiogram findings, whereas in cohort A, the treatment was performed according to the European Association of Urology guidelines: tetracyclines (doxycycline) or levofloxacin [11]. Partners were treated as well, and the use of condoms was advised to all patients in cohort B during the antibiotic therapy, as is common practice in our center. All patients with persistent infection by the same pathogen at the posttreatment microbiological evaluation were excluded. On the other hand, not all patients with recurrent infection were excluded. We compared the two cohorts of patients considering the following parameters:
7. Statistical and ethical considerations
As a null hypothesis, we assumed that there was no significant difference between cohorts A and B in terms of number of symptomatic recurrences per patient and mean score on all the questionnaires. For sample characterization and assessment of the distribution of scores, descriptive statistics were used, including measures of central tendency (mean) and dispersion (standard deviation) for quantitative variables and frequency for categorical variables. All variables were subsequently coded for analysis as continuous or categorical in accordance with their characteristics. Data were presented as the mean±standard deviation. We compared the 2 cohorts at enrollment by using a 2-tailed Student t-test for paired/unpaired data and a chi-square analysis for the comparison of proportions. All variables of interest were collected during urological examinations and recorded in a dedicated database (Advanced PROSTATitis DataBase, Microsoft Access format). Statistical significance was achieved in the presence of an alpha-error inferior to 0.05. All reported p-values were 2-sided. All data were recorded, collected, and analyzed by using IBM SPSS 20.0 for Apple-Macintosh (IBM Co., Armonk, NY, USA). The local research ethics committee approved the present study (Department of Urology; University of Florence; URO_Datac3_2007), and written informed consent was obtained from all patients before their enrollment. The study was conducted in line with Good Clinical Practice guidelines and in line with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement (http://www.strobe-statement.org).
RESULTS
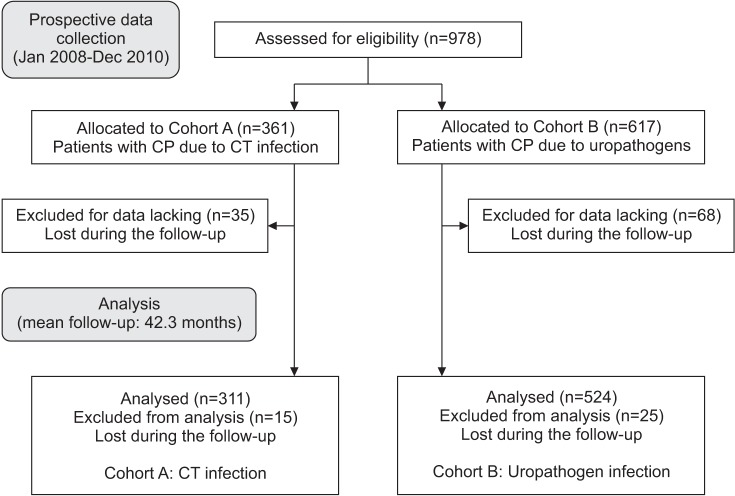
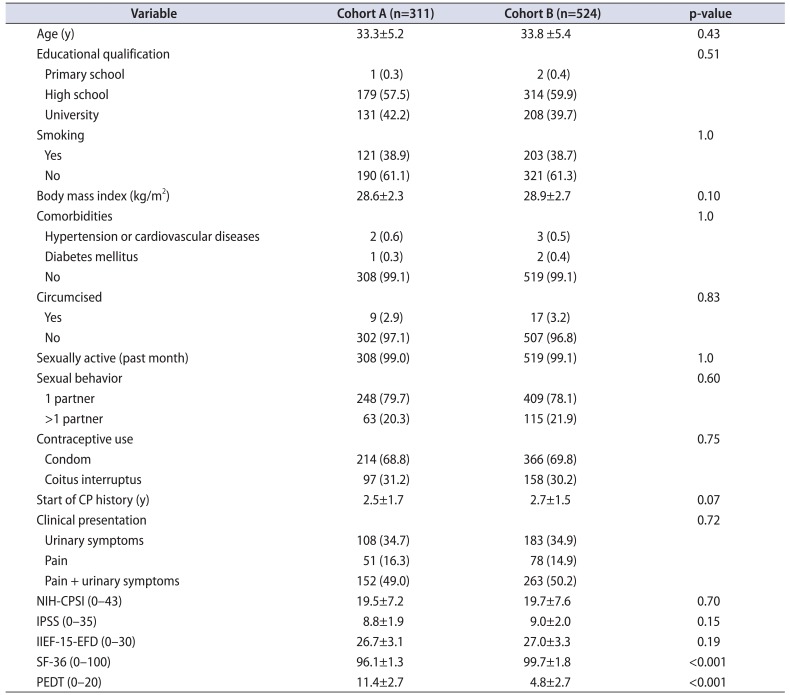
From a total population of 3,127 consecutive patients attending our STI centre with a confirmed diagnosis of CBP (category II, NIH classification) with symptoms lasting >6 months, 978 patients were considered eligible for the study. One hundred three patients were excluded for lack of data collection and 40 were lost to follow-up. In the end, 835 Caucasian patients (mean age, 33.6±7.1 years) were enrolled: 311 in cohort A and 524 in cohort B (Fig. 1). Anamnestic and clinical data at enrollment are shown in Table 1. The 2 cohorts of patients were comparable in terms of age and clinical characteristics. At the time of enrollment, the 2 cohorts had comparable distributions of NIH-CPSI (p=0.70), IPSS (p=0.15), and IIEF-15-EFD (p=0.19) scores. Compared to cohort B, cohort A had significantly worse scores on the PEDT test (11.4±2.7 vs. 4.8±2.7, p<0.001) and lower scores on the SF-36 tool (96.1±1.3 vs. 99.7±1.8, p<0.001).
1. Microbiological results at the time of enrollment
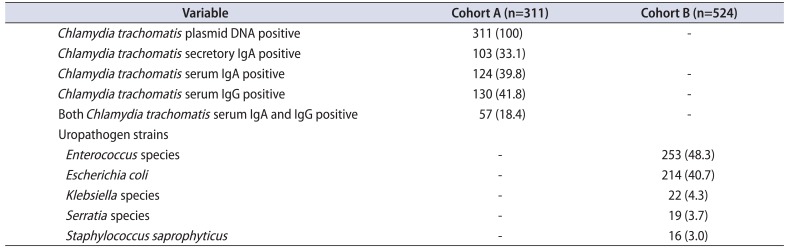
From the 835 studied cases, 2,765 genitourinary samples were collected and analyzed. Three hundred eleven patients (37.3%) had positive results for mucosal anti-CT IgA in urogenital samples and/or CT-DNA but had negative results for cultures for other bacteria or yeasts. These patients were allocated to Cohort A. Five hundred twenty-four patients (62.7%) had positive results for common uropathogens but not for CT and were allocated to Cohort B. Table 2 lists the microbiological findings in both groups.
2. Treatment at the first evaluation and at the end of the study period
At the first evaluation, all patients in cohort B had been treated in line with the microbiological results. The most commonly used antibiotics were levofloxacin (378 of 524, 72.1%), ciprofloxacin (102 of 524, 19.5%) and cotrimoxazole (25 of 524, 4.7%). In cohort A the most commonly used antibiotic was doxycycline (289 of 311, 92.9%). The median treatment time was 4 weeks in cohort A and 2 weeks in cohort B.
At the end of the study period, the most commonly used antibiotics in cohorts A and B were the same as shown in the first evaluation.
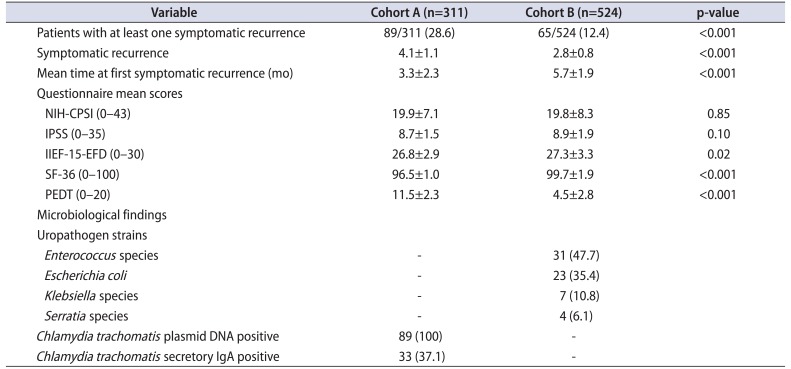
3. Clinical evaluation, questionnaire, and microbiological results at the end of the study period
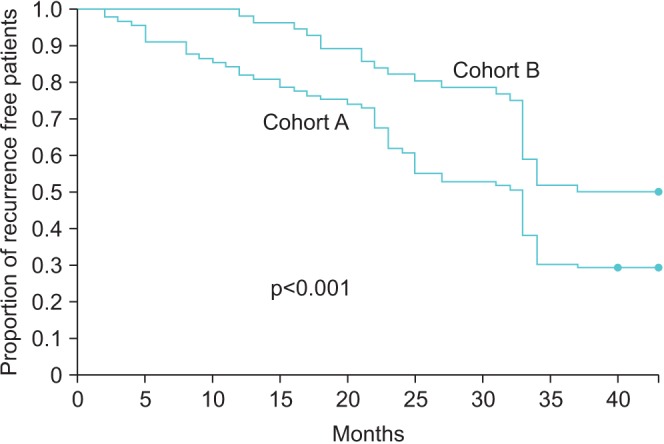
After a mean follow-up of 42.3 months, cohort A showed a significantly higher number of symptomatic episodes than did cohort B (4.1±1.1 vs. 2.8±0.8, p<0.001) and a shorter mean time to first symptomatic recurrence (3.3±2.3 months vs. 5.7±1.9 months, p<0.001). Fig. 2 shows the Kaplan-Meier curves of the risk of recurrence in the 2 cohorts. Compared to cohort B, cohort A showed significantly worse scores on the SF-36 tool (96.5±1.0 vs. 99.7±1.9, p<0.001), IIEF-15-EFD (26.8±2.9 vs. 27.3±3.3, p=0.02), and PEDT questionnaire (11.5±2.3 vs. 4.5±2.8, p<0.001) at the end of the follow-up period. No significant differences in terms of urinary symptoms were reported on the IPSS (8.7±1.5 vs. 8.9±1.9, p=0.10) or NIH-CPSI (19.9±7.1 vs. 19.8±8.3, p=0.85). Table 3 shows all clinical and microbiological results at the end of the follow-up period.
DISCUSSION
In the present study we focused our attention on the natural history of CBP due to CT infection, hypothesizing that the clinical characteristics of patients affected by CBP due to CT infection would differ from those of patients with CBP due to common uropathogens. We hereby demonstrated that patients with CBP due to CT infection reported a higher number of symptomatic episodes with a shorter mean time to first symptomatic recurrence. Moreover, patients affected by CT infection reported lower scores on the SF-36, IIEF-15-EFD, and PEDT questionnaires, demonstrating a higher impact on the patient's quality of life.
The impact of bacterial strains on the clinical outcome of patients has not been analyzed in depth. Several authors have demonstrated the role of CT as a causative pathogen, but to date no study has been performed to demonstrate the role of bacterial type in the natural history of the disease. On the one hand, Park et al. [20] demonstrated that the presence of CT infection is associated with a higher pain score and can worsen quality of life in patients with chronic prostatitis or chronic pelvic pain syndrome (CP/CPPS). On the other hand, Cai et al. [7] demonstrated that patients affected by CBP due to CT infection reported a higher prevalence of premature ejaculation and a lower sexual quality of life. In this sense, the presence of CT infection should be considered as a risk factor for a worsened general and sexual quality of life. Mazzoli et al. [5], in addition, highlighted the fact that the level of mucosal anti-CT antibodies (mucosal IgA) is correlated with interleukin (IL)-8 levels and symptom scores in patients with CP/CPPS. Moreover, patients with higher levels of IL-8 and higher positivity for mucosal IgA reported the worst symptoms [5]. Koroku et al. [21] also demonstrated that the presence of CT infections is related to a higher rate of white blood cells in EPS in CP/CPPS patients. In our population, we found that patients with CBP due to common uropathogens showed a lower number of symptomatic episodes in the whole study period than did patients with CBP due to CT (2.8 vs. 4.1). The natural history of CBP due to common uropathogens is quite similar to that shown by Nickel et al. [22] in a 1-year follow-up study. Nickel et al. [22] demonstrated that 63% of patients experienced persistent symptoms and reported at least one symptomatic episode in 12 months. The same results were also reported by Turner et al. [23]. The symptomatic recurrences observed in the cohort of patients affected by CT infection are probably due to the fact that the microbiological eradication and the clinical cure are not optimal; Skerk et al. [24] reported an eradication rate of about 80% of all patients treated with azithromycin.
There were several important strengths to our study. The first was the prospective nature of the study design and the large patient population. The fact that all patients were evaluated in a single center is another strength; as a result, the patient selection and evaluation criteria were the same, as were the microbiological evaluation and follow-up visits. CT is a rare and nontraditional pathogen in CBP. In this study we performed an accurate microbiological assessment by using urethral swabs to exclude all patients with urethritis. Moreover, the long-term follow-up period was another point that gave strength to the study. It is well known that sexual function and other prostatitis-like symptoms can be related to age, smoking, or other clinical characteristics. Our cohorts of patients were homogeneous in terms of sociodemographic, anamnestic, and clinical characteristics. In this sense, the differences between the two groups in terms of sexual function were fully correlated to CT infection.
On the other hand, a few limitations should be taken into account. First, our study population was composed of patients referred by second- or third-level specialized centers. It is also true that we analyzed a large cohort of patients and this might reflect various clinical scenarios found in a more general patient population. We highlight that assigning sexual function status solely on the basis of IIEF and PEDT questionnaires could be considered a limitation of this study. Some authors have argued that the specificity of questionnaires is relatively low as a reliable tool in diagnosing male sexual dysfunction [25].
This study highlights 2 key aspects to consider in everyday clinical practice: the presence of CT infection in patients with CBP should be considered as a marker associated with a worse clinical outcome. Chlamydia infection is a common STI. Patients with this strain are questioned about a low IIEF-15-EDF score and a high PEDT score. Therefore, diagnostic tests for CT are highly recommended for patients with prostatitis-like symptoms. The treatment, even when carried out in line with the European Association of Urology guidelines or international recommendations, cannot prevent the risk of new recurrences. It is likely that antibiotic therapy cannot fully eradicate the infection, especially when faced with an intracellular pathogen located in prostate tissue. For this reason, greater attention should be given to those patients with a known history of CT infection because they carry a greater risk of early recurrence, even if the results of microbiological analysis after the first treatment are negative.
CONCLUSIONS
In conclusion, patients affected by chronic prostatitis due to CT have a higher number of symptomatic recurrences that more severely impair general and sexual quality of life compared with patients affected by chronic prostatitis caused by traditional uropathogenic bacteria. Additional prospective studies are needed to clarify the role of inflammation and infection of the prostate gland due to CT and other pathogens.
 XML Download
XML Download