

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Prostate cancer is the most common type of cancer, and is the second leading cause of cancer-related mortality among men in Western countries [1]. However, in Asian countries the incidence of prostate cancer is lower [2]; for example, prostate cancer is the fifth most common cancer among men in Korea [3].
However, the incidence of prostate cancer in Korea is rapidly increasing. According to the Korea National Cancer Incidence Database, the age-standardized incidence rate of prostate cancer in males, which was 8.4 per 100,000 in 1999, reached 26.2 per 100,000 in 2013. The annual percent change in prostate cancer was 11.4%; the second largest increase observed, following thyroid cancer [3]. Thus, prostate cancer has become one of the most important cancers to consider in Korean elderly men.
Currently, there exists a nationwide, training hospital-based cancer registry (the Korea Central Cancer Registry, KCCR). This registry includes the annual prostate cancer number, incidence, prevalence, mortality, and information on survival [4]. However, there is no information regarding clinical stage or treatment data in this registry. Therefore, KCCR data is useful for the government in making national policies, but not so in making treatment-related decisions, on an individual level, by Korean urologists.
Most of the current known guidelines for prostate cancer were made in Western countries and are based on their countries' respective data. However, the characteristics of prostate cancer vary according to race and region [5]. For the optimal diagnosis and treatment of Korean patients with prostate cancer, the collection of detailed Korean prostate cancer data, including clinicopathological data is necessary. However, the KCCR does not provide such type of data. Therefore, the Korean Urological Oncology Society (KUOS) introduced another database called the Korean Prostate Cancer Database (KPCD), where it would be possible to find such data.
In this article, we aimed to describe the protocol of data collection for the KPCD and to present the gross results of Korean prostate cancer characteristics obtained from the database.
Go to : 
MATERIALS AND METHODS
1. Organization of KPCD
The decision to form the KPCD program was made in 2010. At first, the KUOS organized a task force team to assist in the development of the database. After several task force team meetings, the database protocol, timeline, and participating institutions were agreed upon.
Following the consideration of regional distribution, 20 hospitals were selected to participate in the creation of the KPCD. The following institutions (in alphabetical order) participated: Asan Medical Center, Chonbuk National University Hospital, Chonnam National University Hwasun Hospital, Chungbuk National University Hospital, Dong-A University Hospital, Eulji University Hospital, GangNeung Asan Hospital, Inha University Hospital, Inje University Pusan Paik Hospital, Keimyung University Hospital, Konkuk University Chungju Hospital, Korea University Anam Hospital, Kyungpook National University Medical Center, National Cancer Center, Pusan National University Hospital, Samsung Medical Center, Seoul National University Hospital, Seoul National University Bundang Hospital, and Yonsei University Severance Hospital.
2. Data collection
The database protocol was decided upon in January of 2012. This protocol consisted of 4 domains (demographic, pretreatment, treatment, and follow-up data) and 135 variables. Specifically, demographics (patient age); pretreatment data (date of diagnosis, prostate-specific antigen [PSA], free PSA, digital rectal examination findings, biopsy findings such as Gleason score, computed tomography/magnetic resonance imaging findings, bone scan findings, metastasis information, and clinical stages); treatment data (active surveillance, operation, radiation therapy, hormone therapy, neoadjuvant therapy, and adjuvant therapy); and follow-up data (date of last follow-up, nadir PSA, biochemical recurrence, salvage treatment, disease progression, cancer-specific survival, and overall survival), were all recorded and analyzed.
The subjects involved in the KPCD were all patients with biopsy-proven prostate cancer from 2000 to 2010. Data collection was performed twice. Data collection started in February of 2012, and all patients with biopsy-proven prostate cancer from 2000 to 2005 were enrolled. The data of 2,018 patients were collected during 2012. After the first data analysis, the task force team corrected several points of the database protocol. The second set of data collection was commenced in 2013, targeting patients who were diagnosed as having prostate cancer from 2006 to 2010. The data of an additional 5,590 patients were collected in 2013. The collection and analysis of all data were approved by the Institutional Review Boards of all 20 hospitals that participated in the KPCD (approval number: 2015-1384).
3. Statistical methods
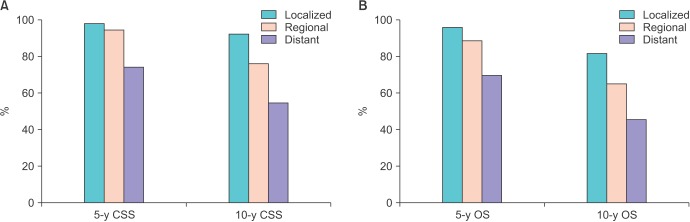
All statistical analyses were performed using IBM SPSS Statistics ver. 19.0 (IBM Co., Armonk, NY, USA). Continuous variables are presented as mean±standard deviation. Categorical variables are presented as number and percentage. Kaplan-Meier analysis was used to calculate the 5-year and 10-year cancer-specific survival and overall survival rates, respectively. To compare the survival results according to clinical stage, the prostate cancer status at diagnosis was categorized as localized (≤cT2 and N0 without metastasis), regional (≥cT3 or N1 without metastasis), and distant (any T and any N with metastasis).
Go to :
RESULTS
In total, 7,608 men with biopsy-proven prostate cancer, identified from 2000 to 2010 were registered in the KPCD. The mean age at diagnosis was 67.6±7.7 years. The mean PSA at diagnosis was 74.0±366.9 ng/mL, and the proportions of patients with Gleason scores≤6, 7, and 8–10 were 37.0%, 26.7%, and 34.2%, respectively. At diagnosis, 62.3% of patients had localized tumors, 14.6% had regional tumors, 12.8%, had distant tumors, and 10.4% had unknown diseases. With respect to the initial treatment modality, 1.3% of patients were managed with active surveillance, 62.1% underwent surgery, 4.3% underwent radiotherapy, 27.1% underwent androgen deprivation therapy, and 5.2% had unknown treatments. The clinical and pathological characteristics of these patients are summarized in Table 1.
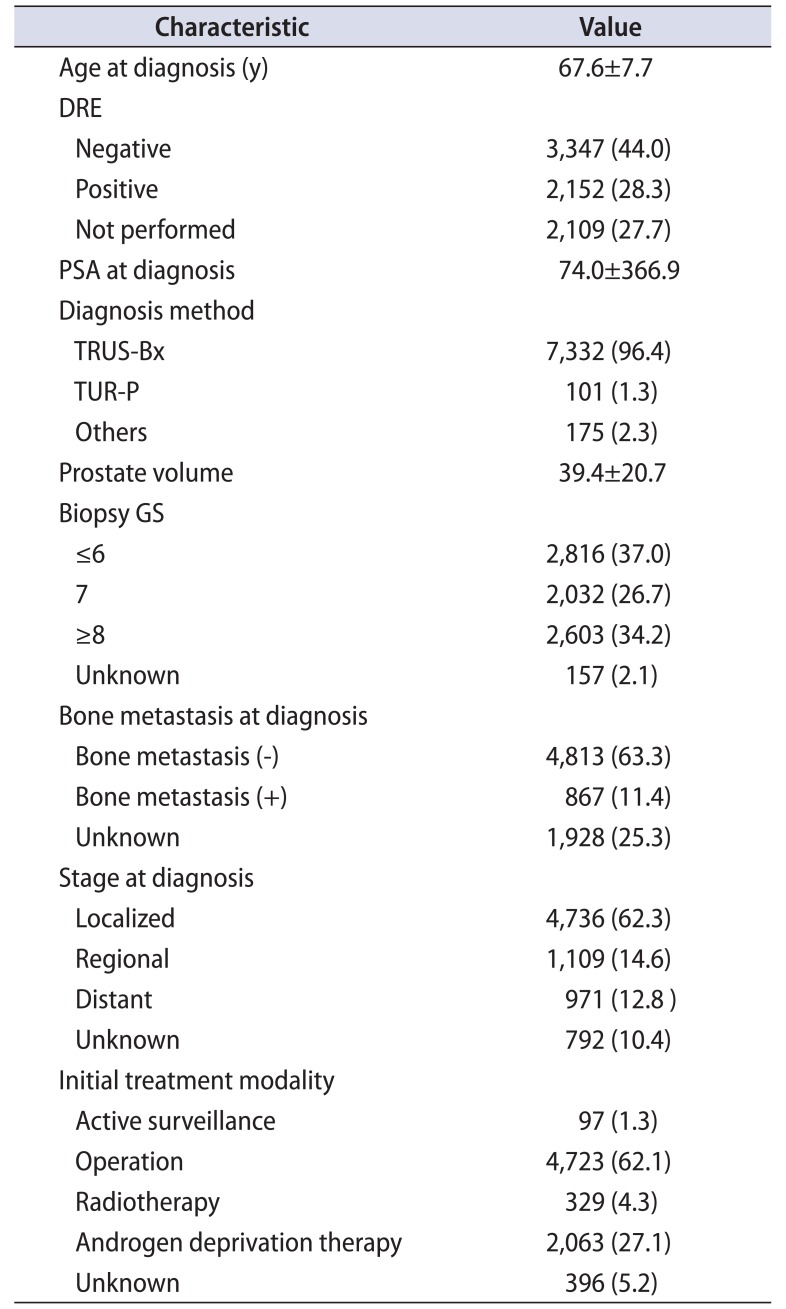
Table 1
Clinical and pathological characteristics of patients in Korean prostate cancer database (n=7,608)
![]()
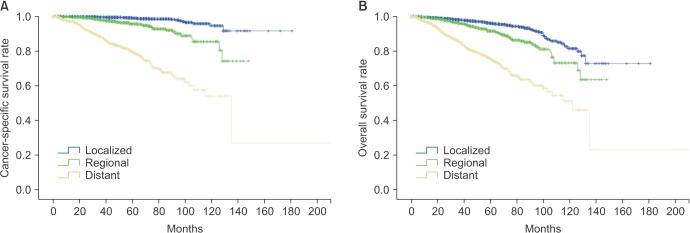
The 5-year cancer-specific survivals of patients in the KPCD were 98.6% in the localized stage, 94.8% in the regional stage, 74.7% in the distant stage, and 86.9% in the unknown stage. The survival data of these patients are summarized in Figs. 1, 2.
Go to :
DISCUSSION
In Korea, the prevalence of prostate cancer has quadrupled from 2002 to 2008, and the increased incidence rate is highest in terms of total forms of malignancy [6]. Despite this rapid increase in the number of patients with prostate cancer, there is no established representative data for prostate cancer in Koreans. The characteristics of prostate cancer vary according to race and region [5]. Therefore, the most appropriate approach for the management of prostate cancer in each country probably also differs. This is the main reason that detailed prostate cancer databases, including clinicopathological data, in each country exist, such as the Cancer of the Prostate Strategic Urologic Research Endeavor (CaPSURE) in the United States and the Japan Study Group for Prostate Cancer (J-CaP) in Japan [78].
The KUOS was established in 1990. The purposes of KUOS at its establishment were the improvement of clinical and basic research and the exchange of knowledge regarding urological oncology. In agreement with these purposes, KUOS decided to gather established representative data for prostate cancer in Koreans.
The KPCD was made by retrospectively reviewing medical records. The data of 7,608 Korean patients with prostate cancer diagnosed from 2000 to 2010 were collected. Compared with CaPSURE, which consists of approximately 14,000 registered patients with prostate cancer, and J-Cap, which consists of 17,872 patients, this is a small database [78]. However, this database represents the largest data set for Korean prostate cancer to date, and it can be further updated in the future. We trust this is an important first step for the appropriate management of prostate cancer in Koreans.
For a similar purpose, the multicenter Korean Prostate Cancer Database (K-CaP) was created in 2011 [9]. These two databases consist of different centers and somewhat different protocols. However, we hope that these two databases will maintain a cooperative and complementary relationship with each other.
In Korea, there is a KCCR managed by the government [4]. This registry includes no information regarding clinical staging or treatment data; however, it is a nationwide registry and includes reliable annual prostate cancer numbers, as well as information on incidence, prevalence, mortality, and survival. The 5-year relative survival rate according to the KCCR was 90.2% from 2006 to 2010. The 5-year relative survival rate according to the SEER from 2002 to 2008 in the United States was 99.2%. The 5-year cancer-specific survival rate of our database (from 2000 to 2010) was 94.3%. Our data is higher than the KCCR but lower than the SEER. In the authors' opinion, our database has more detailed data than the KCCR, so it provides a more reliable estimation of cancer-specific survival rates in Koreans. A more detailed survival data comparison between our data, KCCR, and SEER is summarized in Table 2 [1011]. It was interesting to find that the 5-year survival based on our data and KCCR in the localized and regional stages were similar, while they were noticeably different in the distant stage. In the distant stage, the 5-year cancer-specific survival based on our database was 74.7%, but the same stage had a survival rate of only 36.4% in the KCCR. At this point, we are unable to discern the reason; however, one possible explanation for this difference could be poor mortality data. Our mortality data were obtained from only medical records of each hospital, not Statistics Korea. Thus, it was possible we missed mortality data. Other differences were found between the distant stage rate and the unknown stage rate (13% vs. 9% at the distant stage; 10% vs. 18% in the unknown stage). Our database may be more reliable because it consists of detailed data.
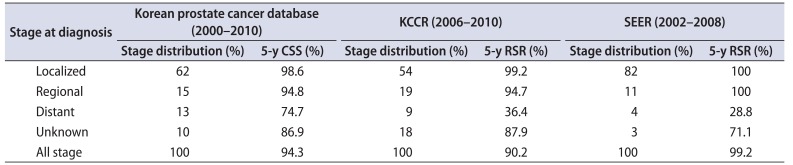
Table 2
Comparison of 5-year relative survival rates (RSRs) for prostate cancer with Korea Central Cancer Registry (KCCR), Surveillance, Epidemiology, and End Results (SEER) in the United States and 5-year cancer-specific survival (CSS) rate in the Korean prostate cancer database
![]()
However, there are many limitations of our database as well. First, our database consisted of nonhomogeneous data. This is a multicenter database with 20 participating hospitals. So, patient number, reliability, and quality of data in each center is different. To overcome this limitation, a single reviewer evaluated the data as a whole, and excluded several unreliable data points. Moving forward, we will concentrate our efforts on quality control in each center. Second, our data cannot properly represent all Korean patients with prostate cancer. Although we tried including most of the big centers with consideration of the regional distribution, our data is but a small part of the total number of Korean patients, and individual patient characteristics can vary greatly due to the big center-oriented nature of our data.
Despite these weaknesses, the establishment of the KPCD by the KUOS is an important first step in identifying trends in prostate cancer in Korean. KUOS will continue to do their best to improve and extend the KPCD. We trust that the KPCD will become a representative Korean database, similar to other databases in other countries like SEER, CaPSURE, and J-Cap.
Go to :
CONCLUSIONS
The KUOS introduced an established database for Korean prostate cancer in 2010. Data from a total of 7,608 Korean patients with prostate cancer from 2000 to 2010 were collected successfully. The KPCD will be proceed continuously until it becomes a representative Korean database from which clinicians can draw valuable information.
Go to :
 XML Download
XML Download