

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Approximately 7% of men worldwide are affected by male infertility, of which male factors contribute to 40%–50% of all infertility cases [1]. The basic semen analysis remains as the standard of care to initially evaluate male infertility despite its controversies in clinical effectiveness [23]. The test yields highly variable results from the same individual, inconsistent semen parameters among different observers, and no information about sperm dysfunctions at the molecular level. Additionally, the 2010 World Health Organization's reference values might not be applicable to all men as their inclusion criteria lacks diverse patient populations [4]. Therefore, more advanced tests of sperm function may assist in accurately diagnosing male infertility.
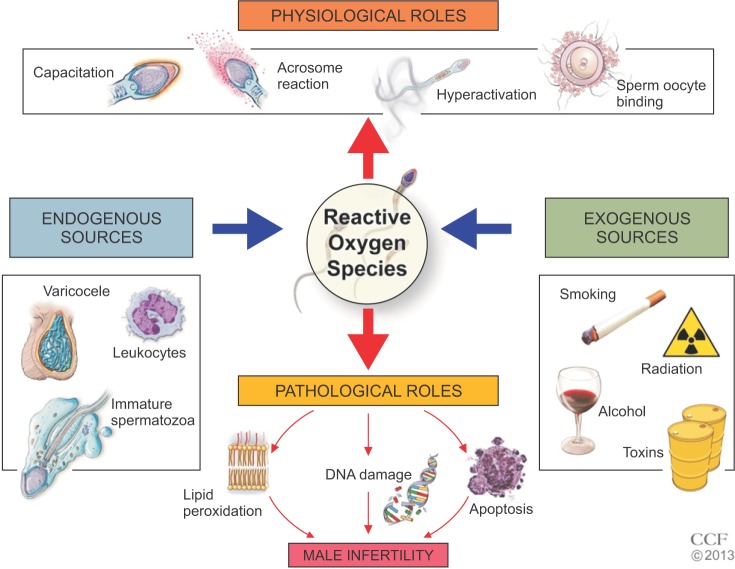
Oxidative stress (OS) is highly implicated in the pathogenesis of male infertility [5678]. OS occurs when production of reactive oxygen species (ROS) outweighs the concentration of antioxidants in human semen. Physiologically, ROS are vital for sperm maturation as they undergo capacitation, hyperactivation, acrosome reaction, and oocyte fusion [910]. However, excess ROS results in lipid peroxidation, DNA damage, and induction of apoptosis, all of which trigger a vicious cycle of OS [11]. Clinically, OS can translate into reduced fertilization rates, failure of implantation, impaired embryonic development, recurrent pregnancy loss and poor assisted reproductive technology (ART) outcomes [121314151617].
Early and accurate detection of OS ensures a better prognosis for infertile men. Currently available assays include chemiluminescence for ROS, total antioxidant capacity (TAC) for antioxidants, and malondialdehyde (MDA) assay for post hoc damage from lipid peroxidation. However, these tests carry certain disadvantages such as high cost, sophisticated instrumentation, large sample volumes, complex methodologies, and extensive technical training [1819202122] (Supplementary Table 1). Most importantly, they only capture a single dimension of OS, quantifying either ROS or antioxidants. Thus, a test that includes all of the constituents of OS may provide a better understanding of the true redox state and facilitate better management.
Measuring oxidation-reduction potential (ORP) is the latest advancement in male infertility diagnostics. ORP, also known as the redox balance, is a direct measure of OS as it describes the relative proportions of oxidants (ROS) to reductants (antioxidants). Previous clinical studies have been successful in evaluating ORP in the blood of patients with traumatic brain injury, stroke, metabolic syndrome, liver toxicity, sepsis, and exercise-induced OS [232425262728293031]. ORP measurement has recently been tested in human semen by a number of andrology laboratories to determine whether it is a reliable indicator of OS. The objective of this review is to (1) describe the causes and mechanisms of OS-induced damage in male infertility; (2) briefly discuss the mechanics of the MiOXSYS System, a device that measures ORP; (3) summarize the data produced by recent clinical studies; and (4) introduce studies in progress that may pave the way for utilization of ORP in clinical practice.
CAUSES AND MECHANISMS OF OXIDATIVE STRESS-INDUCED DAMAGE IN MALE INFERTILITY
There are multiple endogenous and exogenous factors responsible for poor sperm quality in an infertile man. They cause infertility by producing a surplus of ROS targeted towards healthy spermatozoa. Examples of conditions that elevate ROS include: genital tract infections, varicocele, spinal cord injury, diabetes, obesity, tobacco smoking, alcohol use, recreational drug abuse, ionizing radiation, psychological stress, strenuous exercise, or air pollutants [323334] (Fig. 1). Two major sources of ROS are leukocytes via the hexose monophosphate shunt and immature spermatozoa at the level of the plasma membrane or mitochondria [35].
Spermatozoa are highly susceptible to ROS due to the specific composition of their plasma membrane. They contain polyunsaturated fatty acids, which are structurally unstable and highly prone to lipid peroxidation [36]. Electrophilic aldehyde byproducts, such as MDA, 4-hydroxynonenal, and acrolein, are generated from the peroxidative damage, which negatively affects DNA integrity, mitochondrial function, apoptosis, and cellular signaling [83738]. As aforementioned, the mitochondria are not only a target of ROS, but they are also a major source [39]. Thus, prolonged damage to the inner mitochondrial membrane will create a continuous cycle of ROS production that induces sterility. Overall, there is strong clinical evidence suggesting that OS is linked with male infertility as shown through various meta-analyses of infertile patients with OS risk factors (i.e., varicocele, chronic prostatitis, mobile phone use, cigarette smoking) [4041424344].
MEASUREMENT OF OXIDATION-REDUCTION POTENTIAL: PRINCIPLE OF THE MiOXSYS SYSTEM AND OTHER RELEVANT DEVICES
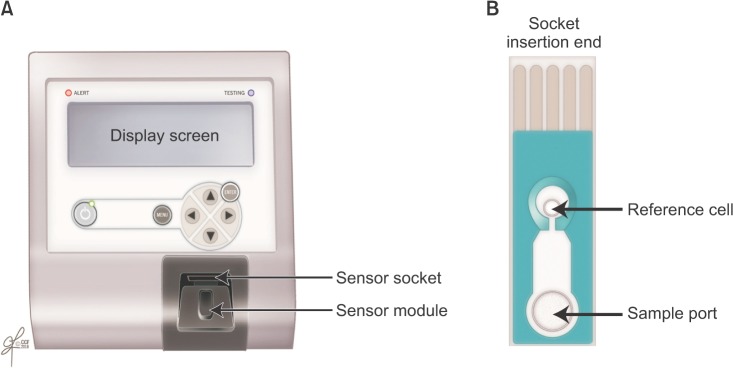
The MiOXSYS System is a novel technology designed to measure the transfer of electrons from reductants to oxidants in human semen samples. ORP is calculated with the Nernst equation: ORP=E°-RT/nF ln([Red]/[Ox]) where E°=standard reduction potential, R=universal gas constant, T=absolute temperature, n=number of moles of exchanged electrons, F=Faraday's constant, [Red]=concentration of reduced species, [Ox]=concentration of oxidized species [45]. To start the procedure, disposable test sensors—each equipped with three electrodes—are inserted into a galvanostatic analyzer (Fig. 2). Once the sample is applied onto the sample port, it will eventually reach the reference electrode, complete the electrochemical circuit, and signal the analyzer to emit a low voltage oxidizing current between electrodes. This current assists in generating an ORP from which the average is calculated from the final 10 seconds of the trial run [46]. The ORP value appears on the analyzer display screen as millivolts (mV), which parallels the degree of OS. A higher ORP corresponds to higher levels of oxidant activity [47].
Similar ORP devices exist in the market but are used to monitor water sanitation, metal finishing, and ozone treatment [4849505152]. To the best of our knowledge, the MiOXSYS System is the first ORP device to test human semen samples. It is specifically calibrated to detect human sperm at 0.1–400 mV. Requiring only 30 µL of sample volume and less than 5 minutes for the entire procedure, the MiOXSYS System yields an ORP value with a high sensitivity, specificity, and accuracy [535455565758]. Fresh or frozen semen and seminal plasma can be also be evaluated [59]. From a technical perspective, the MiOXSYS System is easy to use, inexpensive, less time consuming, and more efficient in providing reliable results. Factors that affect ORP measurement include advanced semen age, poor semen liquefaction, or repeated centrifugation [60616263].
CLINICAL SIGNIFICANCE OF OXIDATION-REDUCTION POTENTIAL MEASUREMENT
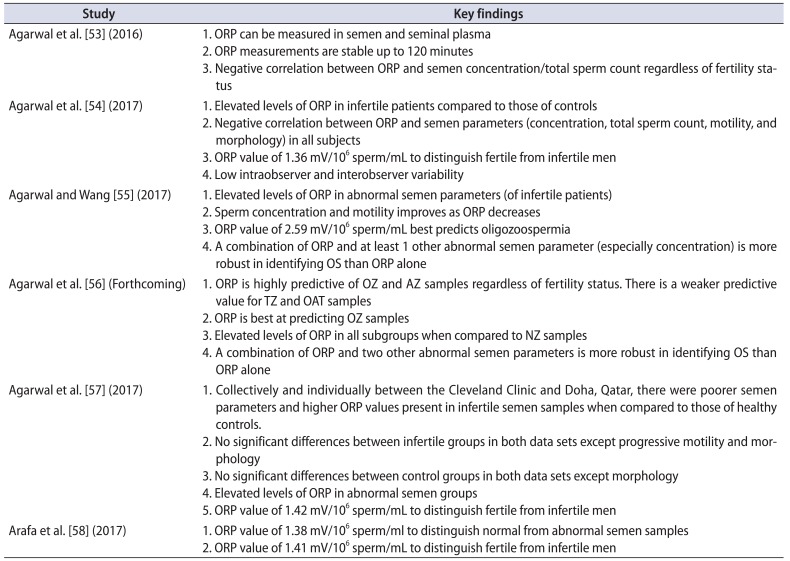
Using the MiOXSYS System, the investigators at Cleveland Clinic's American Center for Reproductive Medicine began measuring ORP to detect OS in human semen samples. Recent clinical studies have generated significant data that enabled ORP measurement to quickly gain momentum as a robust diagnostic tool for male infertility. As a clarification, earlier studies looked at both static ORP (sORP) and antioxidant capacity reserve (cORP) [53]. sORP provides a composite measure of available oxidants and reductants whereas cORP denotes the amount of accessible reductants to combat OS. Due to more promising data, sORP became the topic of interest and was mostly referred to as “ORP” in later studies [54555658]. All studies were conducted with at least a power of 80% with statistical significance set at p<0.05. To calculate ORP (as normalized ORP), the raw ORP value (mV) was divided by the sperm concentration (sperm count × 106/mL). Normalized ORP was expressed as mV/106 sperm/mL. Additional information on the qualitative value of ORP measurement such as its unique ability in predicting abnormal semen parameters and identifying infertile men are elaborated with details of each clinical study published (Table 1).
1. ORP in human semen and seminal plasma
Agarwal et al. [53] initiated a pilot study to measure ORP in human semen and seminal plasma. Another goal of the study was to observe the relationship between ORP and semen parameters across time. The investigators recruited a small cohort of 26 healthy controls and 33 infertile men. Semen samples were analyzed with a basic semen analysis per the 2010 World Health Organization guidelines and ORP measurement at 0 and 120 minutes after semen liquefaction. Compared to those of the controls, semen samples from infertile patients exhibited reduced motility and morphology (p<0.01). Additionally, they had elevated ORP levels in the seminal plasma at 120 minutes (p=0.036). Control and infertile patients were combined and categorized based on normal and abnormal motility (<40%). Individuals with poor sperm motility had lower concentrations, total count, and morphology (p<0.05). Their ORP levels were elevated in semen and seminal plasma at 120 minutes (p=0.035 and p=0.04, respectively). ORP was related to abnormal semen parameters as there was a significant inverse relationship of ORP with concentration and total sperm count at 0 and 120 minutes (p<0.05) (Supplementary Figs. 1,2,3,4). Via a receiver operating characteristic (ROC) curve analysis, an ORP cutoff value of 1.48 mV/106 sperm/mL in semen and 2.09 mV/106 sperm/mL in seminal plasma was proposed to aid in identifying abnormal semen samples, specifically those with <40% motility (Supplementary Fig. 5). Distributions of ORP values and the median in relation to the cutoffs are also displayed in Supplementary Fig. 5. The proposed ROC values were not statistically robust as it yielded low positive predictive values (PPVs) (45% in semen, 46.7% in seminal plasma). This most likely occurred due to a limited number of men with proven fertility in the control group. Including more individuals in the control group with similar baseline characteristics would increase the effectiveness of the assay. Overall, this study demonstrated that ORP can be detected in both semen and seminal plasma up to 120 minutes with the ability to perhaps distinguish abnormal semen quality.
2. ORP in male infertility, establishment of an ORP reference value, and reliability of assay
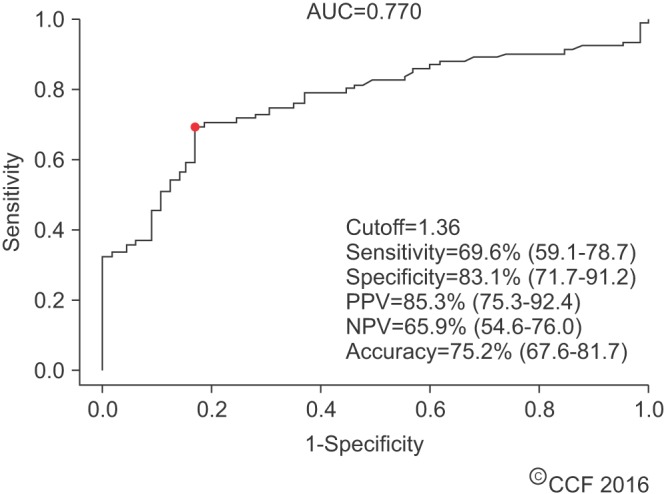
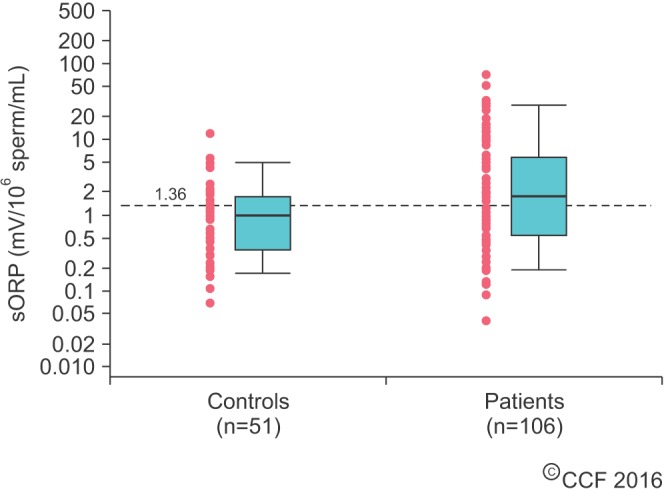
In a second study, Agarwal et al. [54] further attempted to validate ORP as a surrogate marker in predicting abnormal semen. In this study, they enrolled a larger sample of 51 healthy controls (15 proven fertility and 36 unproven fertility) and 106 infertile patients (38 with varicocele, 13 idiopathic, 55 nonclassified). At baseline, the infertile patients had lower sperm concentrations, total sperm count, motility, and morphology (p≤0.001). ORP levels were significantly higher in infertile patients versus controls (6.22±1.10 mV/106 sperm/mL and 1.59±0.29 mV/106 sperm/mL, p=0.004). However, as a collective group, ORP was negatively correlated with concentration, total sperm count, motility, and morphology (p<0.01). ROC curve analysis yielded a normalized cut-off value of 1.36 mV/106 sperm/mL with a 69.6% sensitivity, 83.1% specificity, 85.3% PPV, 65.9% negative predictive value (NPV), and 75.2% accuracy (area under the curve [AUC]=0.770) (Fig. 3). Median ORP values of the infertile patients were above this cut-off value whereas those of the controls were below (p=0.004) (Fig. 4). The same trend was observed when comparing subcategories of patients and controls (Supplementary Fig. 6). Solely measuring ORP appeared to be effective in both determining excess OS in semen samples and differentiating between infertile patients and controls.
Intraobserver and interobserver reliability was tested by having different observers analyze multiple samples in replicates (Supplementary Fig. 7). The goal was to determine if ORP measurement provided more objective data as opposed to conventional semen analysis where high variability is an issue. This was expressed as a coefficient of variation (%CV). Variability for any one observer and across observers were 8.39% and 3.61%, respectively. Overall, this study supported ORP as a highly reproducible measurement and found that a normalized ORP cutoff of 1.36 mV/106 sperm/mL may have discriminative capabilities.
Although ORP values correlated strongly with semen parameters, this study did not further examine whether they were predictive of poor semen quality. This was an important question to answer since ORP in addition to abnormal semen parameters would theoretically be a more robust determination of OS status and male infertility.
3. ORP predictive value and behavior over time in infertile patients
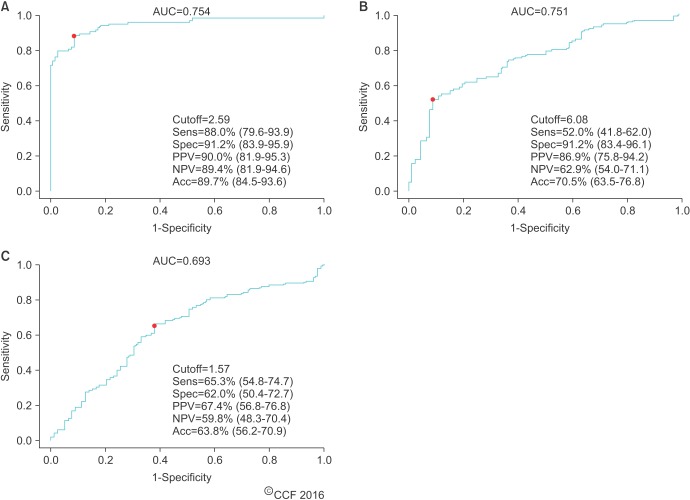
Agarwal and Wang [55] sought to determine the predictive value of ORP and its relationship to semen parameters over time. Semen samples from 49 healthy controls and 194 infertile patients were obtained. Similar to previous studies, the infertile patients had abnormal semen parameters and elevated ORP levels compared with those of the controls (p<0.001). Significant negative correlations between ORP and certain semen parameters were also found in the infertile men (p<0.05). Using the 2010 WHO guidelines, semen samples from the infertile patients were arranged into normal and abnormal semen parameters (oligozoospermia, asthenozoospermia, and teratozoospermia). ORP levels were elevated in all abnormal semen parameters, the highest value belonging to the oligozoospermic group (p<0.001). In fact, ORP was the most predictive of oligozoospermic samples at a cutoff of 2.59 mV/106 sperm/mL with 88% sensitivity, 91.2% specificity, 90% PPV, 89.4% NPV, and 89.7% accuracy (AUC=0.754) (Fig. 5). This coincides with the negative correlation between ORP and concentration. This is also a logical observation since ORP is normalized to concentration.
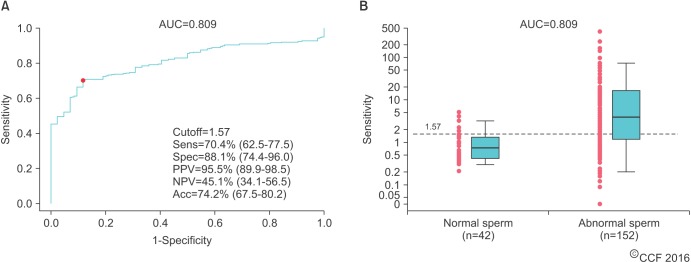
Additional ROC curve analysis demonstrated that an ORP cutoff of 1.57 mV/106 sperm/mL achieving 70.4% sensitivity, 88.1% specificity, 95.5% PPV, 45.1% NPV, and 74.2% accuracy (AUC=0.809) can detect at least 1 abnormal semen parameter (p<0.001) (Fig. 6). There was a greater range of ORP values in infertile patients with abnormal sperm versus that of infertile patients with normal sperm. This suggests that ORP fluctuates as a reflection of abnormal semen parameters induced by OS. Nevertheless, the majority of patients with abnormal semen parameters had an ORP well above the cutoff value.
These reference values confirm prior data showing that ORP is related to semen parameters. Interestingly, because ORP best predicts oligozoospermia, it is very likely that OS strongly plays a pathologic role in this subset of patients [764]. It is important to not forget that OS contributes to other seminal abnormalities as well. This is reflected through different ORP cutoffs for each abnormal semen parameter. This study reveals that a combined approach of considering ORP and at least 1 abnormal semen parameter (especially concentration) is more robust in identifying OS than ORP alone.
To test the relationship between ORP and semen parameters over time, 28 infertile patients underwent repeat semen analyses and ORP measurements at baseline and after 3–5 months. At follow-up, sperm concentration, total motility, and ORP had significantly improved (Supplementary Table 2). This shows that sperm concentration and total motility increase as ORP decreases. Lastly, whether ORP can be used to monitor male infertility due to an infectious agent or inflammatory condition remains unclear. Leukocytes were present in 9 infertile semen samples as verified by the Endtz test and were treated with 200-mg doxycycline daily for 2–3 weeks. Although leukocytes were essentially eliminated, ORP did not show a statistically significant decline.
4. ORP in abnormal semen parameters regardless of fertility status
Agarwal et al. [56] then evaluated the ability of additional combinations of semen parameters and ORP to identify OS regardless of fertility status. The authors also compared ORP levels among different categories of abnormal semen parameters arranged by the 2010 WHO criteria. This study consisted of 15 healthy controls with proven fertility and 293 infertile patients. Comparing infertile patients with controls, there were significant differences in all semen parameters (p<0.05), except for ORP. However, as expected, ORP was negatively correlated with sperm concentration and motility (p<0.0001). Afterwards, healthy and infertile semen samples were grouped altogether and categorized based on abnormal semen parameters (oligozoospermic [OZ], asthenozoospermic [AZ], teratozoospermic [TZ], and oligoasthenoteratozoospermic [OAT]). Normal semen samples were labeled normozoospermic (NZ).
ORP levels were significantly higher in the groups with abnormal semen parameters than in the NZ samples (p<0.0001). Also, ORP was highly predictive of AZ due to the high specificity (86.3%) and PPV (75.3%). This was not the case in regards to TZ. Interestingly, although ORP had a high specificity in predicting OAT, it had a low PPV. This means that an ORP value above the proposed OAT cutoff did not definitively indicate the presence of OAT due to the presence of many false positives. Similar to prior research findings, ORP was best at predicting OZ with a cutoff of 2.63 mV/106 sperm/mL 81.5% sensitivity, 92.7% specificity, 89.1% PPV, 87.2% NPV and AUC=0.919.
Lastly, an ORP cutoff of 2.7 mV/106 sperm/mL can detect at least 2 abnormal semen parameters achieving 64.6% sensitivity, 83.9% specificity, 75.7% PPV, 75.4% NPV and AUC=0.809 (p<0.0001). With this data, clinicians may use a combination of ORP and 2 other abnormal semen parameters to help identify OS rather than using ORP alone. The study results confirmed that ORP measurement is a reproducible test that is highly predictive of abnormal semen parameters regardless of fertility status. Identifying ORP provides a quick composite picture of OS status and abnormal semen parameters in just 1 patient visit. Therefore, the need for multiple follow-ups with patients are not necessary.
5. Reproducibility and reliability of ORP on a global scale
To further test ORP's consistency, a number of studies have used the MiOXSYS System in different ethnic populations at different geographical locations. Agarwal et al. [57] conducted a multicenter retrospective study that compared data from 2 andrology laboratories located in the USA and Qatar for 12 months. Cleveland Clinic, Cleveland, USA, recruited 51 healthy fertile controls and 194 infertile patients. A large tertiary hospital located in Doha, Qatar, recruited 50 fertile controls and 400 infertile patients. The sample population was analyzed as a combined dataset and as individual datasets according to institution. In both data sets and the combined dataset, sperm concentration, total motility, progressive motility, and normal morphological forms were significantly lower and ORP significantly higher in the infertile patients than in the controls (p<0.05). Between the infertile patients of the Cleveland Clinic and Doha, there were no significant differences in ORP or semen parameters except for progressive motility and morphology. Between control patients of the Cleveland Clinic and Doha, there was only a significant difference in morphology (p=0.004).
Data from the combined population and combined number of infertile patients of both institutions were divided into normal and abnormal semen groups according to the 2010 WHO semen parameters. ORP was elevated in both abnormal semen groups (p<0.001) (Tables 2, 3). When combining both study populations, ROC curve analysis generated an ORP cutoff value of 1.42 mV/106 sperm/mL that was able to differentiate fertile from infertile semen groups with 60.6% sensitivity, 74.3% specificity, 93.3% PPV, 24.3% NPV, and 62.6% accuracy (Supplementary Fig. 8). This ORP value persisted even with variations of baseline characteristics such as smoking status, leukocytospermia, age, body mass index, and number of abstinence days.
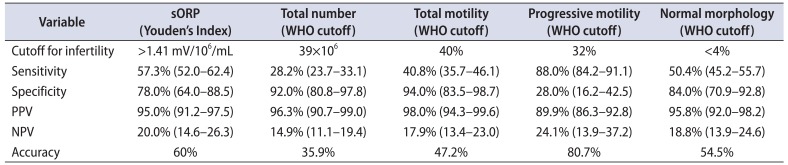
Arafa et al. [58] provided supporting data from Qatar through a prospective study of 365 infertile patients and 50 fertile controls. Decreased semen parameters in all categories and elevated ORP levels were found in the infertile patients (p<0.001) when compared with fertile controls. ORP also showed no significant correlation with age, BMI, or days of sexual abstinence despite differences in those baseline demographics. ROC curve analysis provided an ORP cutoff of 1.38 mV/106 sperm/mL to differentiate normal from abnormal semen quality with a 63.3% sensitivity, 87.8% specificity, 97.6% PPV, 23.2% NPV, and 66% accuracy. A cutoff of 1.41 mV/106 sperm/mL was able to distinguish fertile from infertile men with an accuracy that was better than that of other WHO semen parameters except for progressive motility—a parameter that is quite subjective due to its high intra- and interindividual variability (Table 4).
By enrolling a large number of patients, these studies were instrumental in providing reliable ORP cutoffs that can identify abnormal semen samples and infertile men. Since these values are similar to the ones proposed in previous studies, measuring ORP is a reliable and reproducible technique when analyzing semen samples in diverse populations.
FUTURE DIRECTION OF OXIDATION-REDUCTION POTENTIAL CLINICAL USE
ORP's role as a surrogate marker to aid in the diagnosis of male infertility is under investigation by numerous groups. The following topics were discussed primarily through some recent abstracts presented at national and international medical conferences within the past 2 years. Many of the studies attempted to improve upon previously published papers by recruiting larger sample sizes treating leukocytospermia, monitoring ORP response to treatment, classifying patients according to etiologies of male infertility, and evaluating female factor infertility in the patients' female partners.
1. Relationship to semen parameters
There is convincing evidence that further supports the relationship between ORP and semen parameters. According to Roychoudhury et al. [65], an ORP cutoff of 1.23 mV/106 sperm/mL could identify over 90% of healthy semen samples which was defined as sperm that meets all of the 2010 WHO normal semen parameter criteria. In fact, Elbardisi et al. [66] found that semen with 1 or more poor parameters had higher ORP values than semen that met all of WHO criteria (p<0.05). ORP increased with abnormal semen parameters. Lastly, an ORP cutoff of 1.635 mV/106 sperm/mL had a 98.6% chance of predicting semen with at least 1 or more abnormal semen parameters. Toor et al. [67] observed that ORP was elevated in semen that had a low sperm concentration, low total sperm count, and low sperm motility (p<0.05). There was also a negative correlation with ORP and these parameters (p<0.05). Lastly, Agarwal et al. [68] conducted a multicenter study at 9 institutions around the world with 2010 recruited participants. An ORP cutoff value of 1.34 mV/106 sperm/mL was able to identify samples with abnormal semen parameters with 58% sensitivity, 85% specificity, 96% PPV, 42% NPV, and AUC=0.757. The cutoffs and relationships observed in these studies were similar to the ones established by Cleveland Clinic researchers.
ORP's relationship to sperm morphology is inconsistent. This adds to the controversy of whether to use sperm morphology as an indicator of sperm function [697071]. The aforementioned clinical studies found weak evidence in supporting ORP to predict teratozoospermia [5556]. However, Arafa et al. [72] suggested that a cutoff of 3.29 mV/106 sperm/mL was able to reliably predict abnormal morphology with a 55.6% sensitivity, 89.1% specificity, 85.7.1% PPV, 63.1% NPV and 71% accuracy (AUC=0.90). Additionally, Ayaz et al. [73] found that although sperm morphological abnormalities were present in both fertile and infertile men, they were often found in combination with other semen parameter abnormalities in infertile semen samples. ORP also increased in infertile semen samples as the percentage of sperm neck abnormalities increased.
Total motile sperm count (TMSC) is an excellent semen parameter in predicting severity of male infertility [7475]. Al Said et al. [76] sought to determine a correlation between ORP and TMSC, in hopes that these 2 parameters could provide additional information in the evaluation of male infertility. A significant negative correlation was found (p<0.001). Also, ROC curve analysis showed that an abnormal TMSC (>20 million) can be best predicted with an ORP cutoff of 2.34 mV/106 sperm/mL with a 83.5% sensitivity, 82.5% specificity, 82.9% PPV, 81.4% NPV, and 79.9% accuracy (AUC=0.9). Because of the promising data, this study advocates for concurrent measurement of TMSC and ORP to evaluate male infertility.
2. DNA fragmentation, reproductive outcomes, and ART
Sperm DNA fragmentation (SDF) is most commonly seen in infertile men, which if not detected early, can impair fertilization, embryo development, and successful clinical pregnancy [77787980]. Arafa et al. [81] conducted a prospective study of 312 patients and reported that DNA fragmentation was negatively correlated with total/progressive motility (p<0.001) and positively correlated with abnormal morphology, ORP, and age (p<0.001). Elevated ORP levels were also seen in the semen of the high SDF group compared to that of the normal SDF group (4.03±0.61 mV/106 sperm/mL and 2.14±0.14 mV/106 sperm/mL, respectively, p<0.001).
In a cross sectional study of 1,162 patients, Majzoub et al. [82] observed a positive correlation between the percentage of abnormal sperm heads and levels of ORP (p<0.001) and SDF (p<0.001). This confirms that OS is highly implicated in sperm DNA damage, especially SDF [838485]. In regards to reproductive outcomes, Ayaz et al. [86] observed that the clinical pregnancy rate was higher in patients in a low ORP group (<1.36 mV/106 sperm/mL) than in those in a high ORP group (>1.36 mV/106 sperm/mL) (p=0.006). For ART purposes, monitoring ORP allows for better sperm selection and preparation [87]. Overall, ORP not only detects OS-associated damage, but also provides clues on prognosis which fully informs the clinician on an individual's clinical status.
3. Varicocele
Varicocele is the most common correctable cause of male infertility. Although there are many possible mechanisms of varicocele-induced injury, OS appears to be the main culprit [88]. Agarwal and colleagues observed that ORP levels were higher and semen parameters (concentration, total motility, and morphology) were lower in varicocele patients than in healthy controls (p=0.001) [8990]. ORP was also negatively correlated with concentration, total motility and morphology (p=0.001) [90]. Currently, there is no consensus on the differences of ORP among grades of varicocele—one study found no difference whereas another study stated that patients with a grade 3 varicocele had the highest levels [9091]. Lastly, when compared to patients of idiopathic infertility, varicocele patients had significantly lower sperm concentration, fewer normal morphologic forms, and higher seminal ORP (p<0.05) [92].
4. Leukocytospermia
Genitourinary infections are a major contributor to OS-induced male infertility. Accumulated leukocytes in the seminal plasma (leukocytospermia) increase ROS production and lead to abnormal semen parameters [9394]. In a preliminary study, Sikka and colleagues [9596] proposed monitoring ORP as an indicator of OS in leukocytospermia because ORP values paralleled the levels of certain biomarkers of active inflammation such as the Toll-like receptor 4 and cyclooxygenase 2.
MANAGEMENT OF ELEVATED OXIDATION-REDUCTION POTENTIAL
A clinician should measure ORP in all patients who present to the infertility clinic as an adjunct to the basic semen analysis. As demonstrated in clinical studies, the excellent results show that ORP can provide valuable information about sperm function and a man's fertilization capabilities. This highlights ORP measurement as an important ancillary tool for male infertility evaluation. ORP can be measured to assess patients' initial OS status and to help guide therapeutic interventions. Theoretically, ORP should decrease when the underlying cause of OS is eradicated. Varicocelectomy, antioxidant supplementation, antibiotic treatment, and lifestyle modifications are examples of treatments that may be beneficial in alleviating OS and improving reproductive outcomes [979899100]. This suggests that ORP measurement is perhaps most beneficial for patients with varicocele, idiopathic infertility, and OS-inducing lifestyle habits. Nonetheless, further studies are needed to determine if ORP can be used to longitudinally monitor treatment progress in patients with specific clinical conditions.
CONCLUSIONS
Male infertility is a multifactorial condition in which OS plays a central role. Newer measures such as ORP represent an objective and accurate method that can reliably identify abnormal semen quality and differentiate fertile from infertile men. The ORP test is also a cost-effective and convenient option for patients undergoing evaluation for male factor infertility. ORP measurement has not yet been incorporated into standard clinical practice due to an incomplete understanding of the clinical indications. Its ability to discriminate across different clinical conditions and to monitor therapeutic effectiveness remains unclear. Also, the current evidence is not yet strong enough to advocate for widespread use of ORP as a stand-alone test. Thus, ORP measurement by the MiOXSYS System provides a novel diagnostic method that may be used in conjunction to routine semen analysis with hopes of positively affecting the lives of men burdened by infertility.



 XML Download
XML Download