

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Interstitial cystitis/bladder pain syndrome (IC/BPS) is a chronic disorder characterized by suprapubic pain related to bladder filling, coupled with additional urinary frequency [12]. Frequency in IC/BPS more likely results from fear of pain; therefore, it was thought that patients without pain would show decreased frequency. However, some IC/BPS patients without pain complain of persistent frequency after conventional therapy. Unfortunately, there are no reports about the incidence or risk factors for persistent urinary frequency after conventional IC/BPS therapy.
Although persistent frequency after conventional treatment is annoying, there are no treatment options in the guidelines [13]. While antimuscarinic agents are the mainstay of overactive bladder (OAB) therapy [4], there is no evidence to support their efficacy in the treatment of IC/BPS. Nonetheless, one recent study reported that antimuscarinics had been used in 49% of IC/BPS patients [3]. Therefore, the efficacy of antimuscarinic treatment in IC/BPS patients requires evaluation. We selected patients who had persistent frequency without pain, to eliminate confusion in the assessment of medication efficacy due to pain in IC/BPS.
In the present study, we investigated the incidence of persistent urinary frequency and associated risk factors in IC/BPS patients who had improved pain. In addition, we evaluated the efficacy of antimuscarinic treatment.
Go to : 
MATERIALS AND METHODS
This study was approved by the Institutional Review Board of Asan Medical Center (approval number: S2015-2042-0001). This study followed the Declaration of Helsinki on medical protocol and ethics.
1. Patient selection and conventional treatment for IC/BPS
Our study included 171 patients diagnosed with IC/BPS according to International Continence Society (ICS) guidelines [5], and who had visual analogue scale (VAS) pain scores ≥4, total scores ≥13 on the pelvic pain and urgency/frequency (PUF) questionnaire, and ≥12 on the O'Leary-Sant interstitial cystitis symptom index/problem index (IC-Q). These criteria were used to clearly identify IC/BPS patients. Patient history, symptom questionnaires, and a 3-day voiding diary were also obtained. Urine culture, cytology, cystoscopy, and physical examinations were performed to exclude urinary tract infections, bladder cancer, urinary tuberculosis, urolithiasis, other neurologic diseases, or endometriosis. Voided volume (VV), maximal flow rate (Qmax), and postvoid residual volume were measured by uroflowmetry, while urinary frequency and maximal bladder capacity (MBC) were recorded in 3-day voiding diaries. All treatments were performed according to the guidelines published by the American Urological Association [16]. Conventional treatments included amitriptyline, pentosan polysulfate (PPS), intravesical hyaluronic acid instillation, hydrodistension (HD), or transurethral resection and cauterization (TUR-C), according to the severity of symptoms and presence of Hunner lesions [78].
2. Incidence of persistent frequency
The patients were first divided into 2 groups according to the presence of pain after conventional treatment. Improved pain was defined as lesser than 3 points in VAS after 3 months of conventional treatment. We then identified patients who had persistent frequency which was defined as urinating >10 times/d.
3. Risk factors for persistent frequency
To identify risk factors, we compared baseline clinical variables in patients with or without persistent frequency. The clinical variables analyzed included PUF, IC-Q, and VAS scores, VV, Qmax, MBC, frequency in a 3-day voiding diary, age, and duration of symptoms. By comparing these variables at baseline in the 2 groups, we identified risk factors for persistent frequency. Univariate and multivariate logistic regression analyses were also used to identify independent risk factors for persistent frequency after 3 months of conventional treatment.
4. The efficacy of antimuscarinic treatment
To evaluate the efficacy of antimuscarinic treatment, solifenacin 5 to 10 mg, fesoterodine 4 to 8 mg, or propiverine hydrochloride 20 to 40 mg were given for persistent frequency, and the mean frequency before and after medication was compared. Efficacy was assessed as the reduction in frequency in a 3-day voiding diary after 3 months of medication. Conventional therapy for IC/BPS continued according to patient symptoms and willingness to take medications during this period.
5. Statistical analysis
Statistical comparisons were made using the chisquare test for categorical variables and independent t-test or Wilcoxon rank sum test for continuous variables. Cox proportional hazards method for uni- and multivariate analyses was performed for the determination of risk factors of persistent frequency. Statistical assessments were considered significant when p<0.05. Statistical analyses were performed using IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA).
Go to :
RESULTS
1. Patient characteristics and clinical outcomes of conventional treatment for IC/BPS
Of the 171 patients, 92.9% were female and 7.1% were male. The follow-up duration was 31.1 months (10.4–161.9 months), and the mean duration between symptom onset and diagnosis was 20.5 months (11.1–44.4 months). The mean age of patients at diagnosis was 62.0 years (25–83 years), and mean (±standard deviation) IC-Q, PUF, and VAS scores at diagnosis were 24.2±8.9, 19.6±6.7, and 5.4±2.0, respectively. Conventional therapy was administered according to disease severity: 16.5% underwent TUR-C, 8.2% received HD, 2.5% underwent alternating TUC/HD, 11% had hyaluronic acid instillation therapy with PPS, 43.9% received medication only, and 17.4% underwent combined surgical treatment and PPS. Following these conventional therapies, VAS scores decreased from 5.4±2.0 to 3.5±1.7 at 3 months and 2.1±1.8 at 6 months (p<0.001), and PUF scores changed from 19.6±6.7 to 15.8±6.5 at 3 months and 16.1±6.3 at 6 months (p<0.001). IC-Q scores decreased from 24.2±8.9 to 20.4±9.6 at 3 months and to 19.9±9.5 at 6 months (p<0.001) (Table 1).

Table 1
Baseline characteristics and clinical outcomes in IC/BPS patients after conventional treatment
Values are presented as mean±standard deviation.
IC, interstitial cystitis; BPS, bladder pain syndrome; VAS, visual analogue scale; PUF, pelvic pain and urgency/frequency patient symptom scale; ICQ, O'Leary-Sant interstitial cystitis symptom index/problem index.
a:Baseline vs. 3 months. b:3 months vs. 6 months, variables with statistical significance.
![]()
2. Incidence of persistent frequency
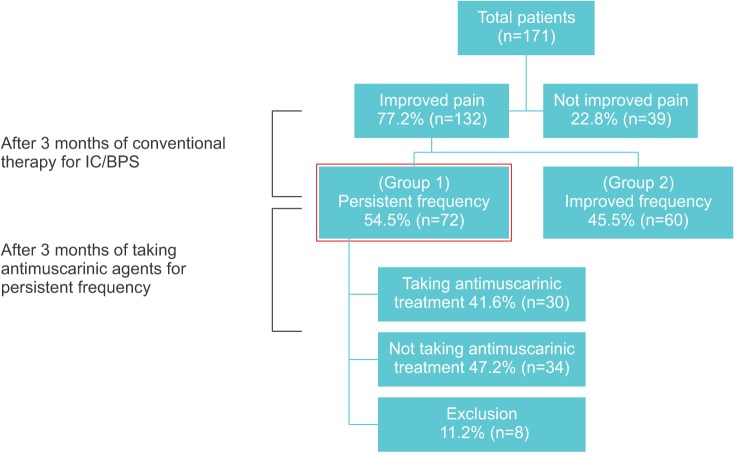
Of the 171 patients, 132 (77.2%) showed improved pain and 39 (22.8%) did not. Among the 132 patients, we identified 72 (54.5%) with persistent frequency, while 60 (45.5%) showed decreased frequency (Fig. 1). There was no difference according to treatment modalities at 3 months between the 2 groups.
3. Assessment of risk factors for persistent frequency
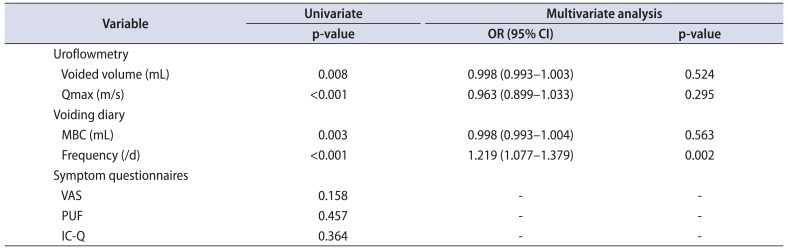
Lower VV (169.7 mL vs. 227.0 mL, p=0.008), lower Qmax (15.7 m/s vs. 21.5 m/s, p<0.001), lower MBC (226.0 mL vs. 284.2 mL, p=0.003), and severe frequency (13.2 times/d vs. 11.5 times/d, p<0.001) at baseline were identified as risk factors for persistent frequency (Fig. 2). Baseline PUF, ICQ, and VAS score did not differ between the 2 groups. Multivariate analysis indicated urinary frequency (p=0.002; odds ratio, 1.219; 95% confidence interval, 1.077–1.379) was an independent predictor of persistent urinary frequency (Table 2).
 | Fig. 2Identification of risk factors for persistent frequency through comparison of groups 1 and 2 with initial variables of bladder function. Group 1, persistent frequency patients; group 2, improved frequency. (A) Voided volume (mL), (B) maximum flow rate (m/s) in uroflowmetry, (C) maximum bladder capacity (mL), (D) frequency (number of micturitions per day) in 3-day voiding diary. All variables are significantly different between 2 groups.
|
Table 2
Uni- and multivariate analyses for predictors of persistent frequency
![]()
4. Evaluation of efficacy of antimuscarinic treatment for persistent frequency
There was no significant difference between patients who took antimuscarinic treatments (n=30) and did not the treatments (n=34) about baseline characteristics, kinds and therapeutic outcome of conventional therapy. The 30 patients who took antimuscarinic medications urinated 14.6±5.6 times/d after conventional therapy, but the frequency decreased to 13.5±4.8 times/d after medication. There was no significant difference before and after medication (p=0.438), and no patient showed a decrease in frequency by more than 20% compared to the baseline before medication.
Go to :
DISCUSSION
The ICS characterizes IC/BPS as a painful bladder syndrome defined by filling-related suprapubic pain accompanied by other symptoms, including increased urinary frequency, without related infection or other previous disease pathology [59]. In IC/BPS, pain and OAB symptoms are the primary problems; there are several treatments for pain but no option for frequency [15]. Hence, urologists usually focus more on pelvic pain and not frequency. One report suggested that urinary frequency associated with IC/BPS results from the fear of pain [10]. The assumed common clinical scenario is that patients show improvement in frequency if pain is improved after conventional IC/BPS therapy. However, in the clinical setting, they still complain of persistent frequency. Unfortunately, there are no reports about the incidence or risk factors for persistent frequency. Moreover, we could not find any reports on the efficacy of antimuscarinic agents for IC/BPS. To our knowledge, this is the first report to identify the incidence and risk factors for persistent frequency, and to evaluate the efficacy of antimuscarinic agents for persistent frequency.
This study made several findings useful in the treatment of IC/BPS patients. First, about 54% of patients showed persistent frequency even though pelvic pain improved after conventional therapy. This is the first report on the incidence of persistent frequency. Second, patients with low VV, low Qmax, low MBC, and severe frequency in a 3-day voiding diary are likely to complain of persistent frequency after conventional treatment for IC/BPS. Moreover, baseline frequency was an independent predictive factor for persistent frequency after conventional IC/BPS treatment in multivariate analysis. These findings correlated with another urodynamic study showing that poor bladder function in IC/BPS patients indicated a higher grade of urothelial dysfunction and a less favorable treatment outcome [11]. These findings are important when we begin treatment for IC/BPS, as poor bladder function can be an important indicator of persistent frequency. Third, antimuscarinic treatment is not useful to treat persistent frequency, as there was no significant difference in the mean daily frequency before and after medication. There is an overlap of symptoms in IC/BPS and OAB. Therefore, IC/BPS patients were usually prescribed antimuscarinic agents, even though guideline for IC/BPS did not include antimuscarinic medication. Interestingly, animal experiments of IC show that antimuscarinic treatment is not effective for detrusor overactivity in a rat model [12]. Meanwhile, patients who had antimuscarinic treatment showed more severe frequency (14.6 times/d) than patients who did not receive medication (12.7 times/d). This suggested that patients who had severe persistent frequency wanted to take medication.
There are several hypotheses regarding the cause of antimuscarinic drug failure in IC/BPS. One study suggested that IC/BPS patients have altered muscarinic receptor expression in detrusor smooth muscle cells [13]. Growing evidence suggests that muscarinic receptor subtype 2 plays a substantial role in detrusor muscle contraction, particularly in an IC/BPS bladder [1415]. Furthermore, another study proposed that urothelial ATP signaling is enhanced in IC/BPS patients [16], while another suggested that activated mast cells release histamine to enhance bladder contractility [17]. Nonetheless, current results will allow urologists to predict which patients will experience persistent urinary frequency before beginning conventional IC/BPS therapy.
Recently, randomized controlled trials and prospective cohort studies have demonstrated that onabotulinumtoxin A is effective for IC/BPS [18]; moreover, another study showed that onabotulinumtoxin A injection decreases urinary frequency from 15.3 to 11.9 times/d and VAS scores from 5.2 to 3.4 after 3 months [19]. Use of β3 agonists for OAB has also increased; however, there is no randomized, controlled, prospective study regarding their efficacy for IC/BPS. Another option, stem cell therapy for OAB and IC, is out of interest. Good results for stem cell therapy in OAB and IC animal models have been reported [2021]. Further research is ongoing for a trial of stem cell therapy in humans.
We evaluated 39 patients who did not show improvement in pain after receiving conventional therapy, and 19 were given antimuscarinic agents due to frequency and pain. Unfortunately, none showed a decrease in frequency after 3 months of treatment, among those who showed no improvement in pain.
Limitations to the present study include its retrospective nature and the small cohort. IC/BPS patients with various degrees and types (Hunner lesion and non-Hunner lesion) were enrolled, it also could be a limitation. However we selected patients who showed improved pain after conventional therapy, we believed that this process might reduce heterogeneity. The number of patients who took antimuscarinic medication was not enough to evaluate the efficacy. However this was the best optimal setting which involved with persistent frequency in order to assess the efficacy of antimuscarinic treatment in IC/BPS. Randomized clinical trials of larger cohorts examining other possible treatments for urinary frequency in IC/BPS, such as β3 agonists and onabotulinumtoxin A injection, need to be conducted in the future.
Go to :
 XML Download
XML Download