

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Because accurately predicting every single occurrence and situation within the human body is near impossible, assuring absolute safety in medical practice is a Herculean task. Outcomes do not always fall within the physician's realm of expectations [1]. Medical accidents come as a surprise to both the physician and the patient and can lead to disputes and possibly litigation. Accordingly, the physician undergoes a vast array of mental and financial stresses from the amount of time spent on selecting legal representation, analyzing medical records in preparation for court, and so on [2]. Furthermore, an increase in litigation arising from medical error encourages physicians to practice defensive medicine, giving way to a simultaneous decrease in quality and an increase in the frequency of medical service [345].
Many studies have been conducted outside of Korea regarding urology-related medical litigation. It is estimated that a licensed urologist comes across an average of 2 malpractice suits during the entirety of his or her career in the United States [67], and one study even revealed that up to 41% of physicians have considered giving up medical practice as a result of the current litigation-prone medical climate [6]. Some research on the subject of medical malpractice litigation has been performed within Korea, including (1) studies that have detailed and classified malpractice cases by the medical department(s) actively involved in the suit [891011], (2) a study dealing with legal issues regarding pulmonary thromboembolism following surgery [12], (3) a study that analyzed malpractice suits regarding postoperative infection after cosmetic surgery [13], and (4) a study that discussed the legal responsibilities of physicians regarding informed consent [14], among others. With respect to research that details and classifies malpractice by the medical department involved, much headway has been made in orthopedics [8], neonatal care [9], cosmetic surgery [10], and anesthesiology [11], with each department showing remarkable variation in the types of liability or fault claimed and the decisions reached in court. However, research regarding malpractice and litigation in Korean urology [15] is insufficient.
Medical dispute and litigation is currently on the rise in Korea [101617]. Damage redress claims for urology-related medical services have remained consistent at 20 to 30 cases filed yearly [17]. It is possible to utilize case files and precedents from previous medical litigation and related analyses as a basic reference for preventing similar incidents from occurring in the future [218]. It was therefore the aim of this publication to understand the characteristics of medical litigation as pertaining to urology by examining court cases surrounding urology malpractice.
MATERIALS AND METHODS
This research took into account a total of 34 urology-related civil proceedings filed within the courts from 2005 through 2010. The Supreme Court of Korea's Written Judgment Management System—a database of cases filed with the Lower Courts, the Appellate Courts, and the Supreme Court of Korea—and its subscription services were utilized to collect case decisions. Researchers from the Asian Institute for Bioethics and Health Law visited the Special Collections Reading Room with special permission from the Supreme Court Library of Korea. The researchers then made inquiries into all cases pertaining to compensatory damages in medical practice from 2005 through 2010. Requests for official copies of the written judgments were then made to the respective courts of delivery, after which electronic copies of said judgments were received by e-mail following redaction of personally identifiable information by the courts. A total of 6,074 cases were received from the courts. The collected judgments were then classified according to medical department. A total of 34 unique cases collected from the Lower Courts, the Appellate Courts, and the Supreme Court were classified as being pertinent to urology malpractice. Additional judgments were requested if substantiation was deemed necessary from cases prior to 2005 and after 2010 to correctly assess the background, the opinion of the court, and the course of the trial.
The researchers compiled and analyzed the following information from the cases: background of the case, age and sex of the patient, categorization of the defendant, the plaintiff's demand, the opinion of the court, the amount claimed in damages, the amount awarded in damages, the type of medical treatment involved, and any negative effects resulting from the medical incident. In cases in which one or more of the factors listed above were not ascertainable from the written judgments provided by the courts, analysis was carried out excluding said factors. Detailed analysis of each case was carried out independently by a urologist (MD) and a doctor of public health (DrPH).
RESULTS
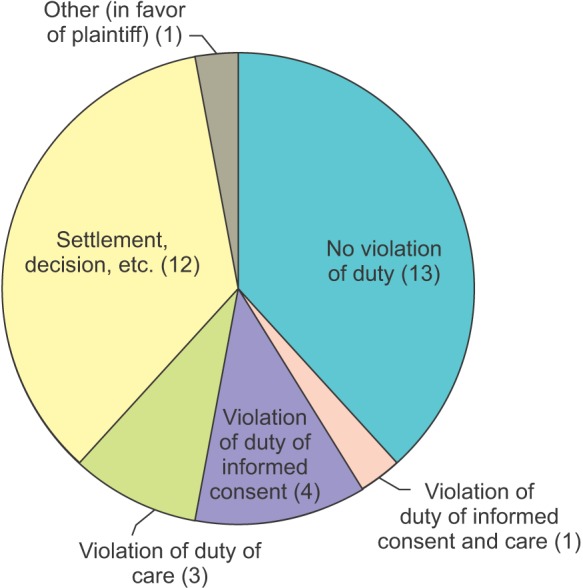
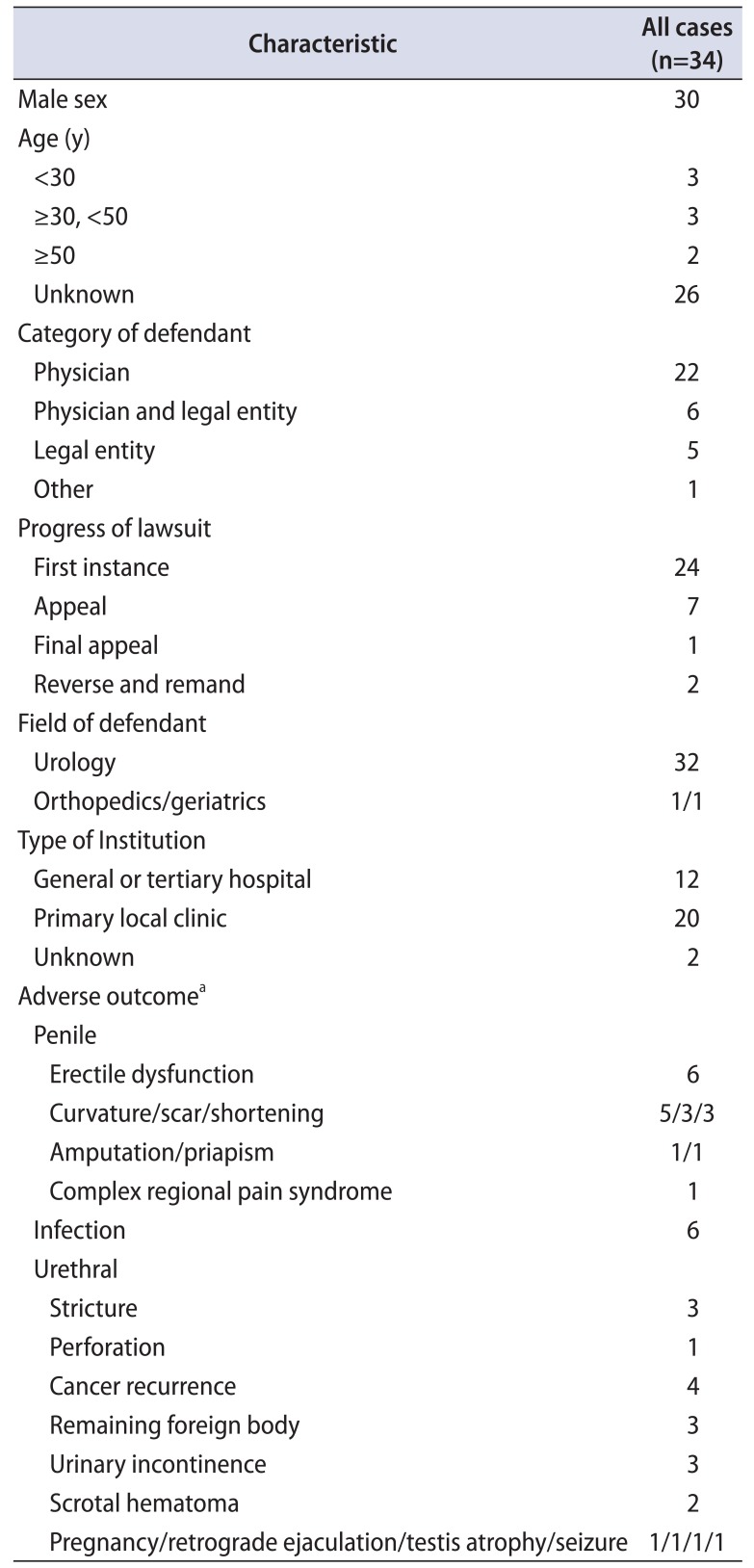
A total of 34 cases of medical litigation involving urology were analyzed in this study. The average period of lawsuits, from the onset of the accident to the end of the litigation, was 3.8 years. All patients, except for 4 cases, were male patients. The patients' ages were ascertainable in eight of the listed cases and varied across the spectrum from 1 year to 68 years. The category of defendant was classified as either “Physician,” “Physician and Legal Entity,” “Legal Entity,” or “Etc.” A total of 20 of the 22 cases classified under the “Physician” category directly involved the attending physician in the legal claim as its defendant, whereas the remaining 2 cases listed both the liable physician and the operator of the employing medical clinic as defendants. In some cases where the claim arose from an accident at a general hospital, both the liable physician and the hospital (as a legal entity) were brought as defendants to court, whereas in other cases, the employing corporation was charged as the defendant. A total of 24 of the 34 cases (70.6%) were resolved at the first instance (Table 1). The average amount claimed was 166,538,543±290,144,414 Korean won (KRW) (5,546,710–1,590,000,000 KRW), and the average amount awarded was 27,186,504±32,371,008 KRW (1,000,000–100,000,000 KRW). Thirteen of the 34 cases (38.2%) were ruled in favor of the defendant, whereas 9 of the 34 cases (26.5%) were ruled in favor of the plaintiff (Fig. 1).
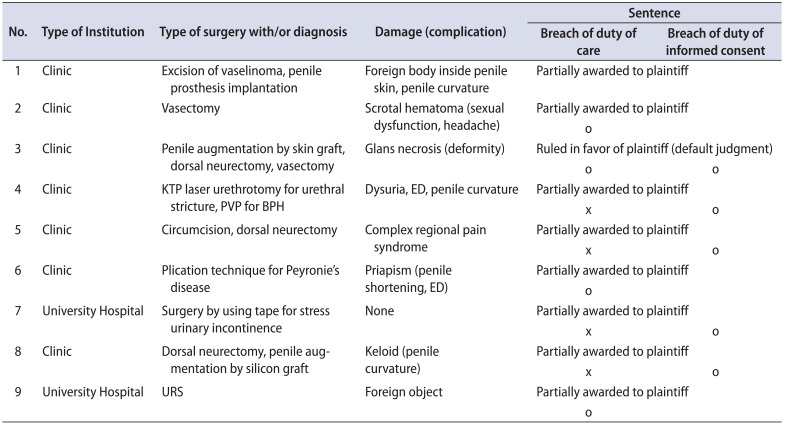
An analysis of the aforementioned nine cases ruled in favor of the plaintiff revealed that the court recognized breach of duty of care owed by the physicians in four cases. One instance dealt with a case (No. 9) in which a foreign object entered the patient's bladder due to negligence while performing ureteroscopic lithotripsy. A second instance (No. 2) involved a breach of duty of care insofar as keeping the vasal artery intact during a vasectomy or suturing the artery immediately in case it is severed during surgery. A third case (No. 3) involved improper treatment of glans necrosis following penile augmentation by skin graft, dorsal neurectomy, and vasectomy. The fourth awarded the case (No. 6) to the plaintiff after the defendant was found negligent in causing damage to the penile arteries during a plication procedure. A miscellaneous case (No. 1) also partially awarded damages to the plaintiff after both parties agreed to settle with regard to any complications that may arise as a result of surgery. All five cases (No. 3, 4, 5, 7, 8) on the ground of breach of duty of informed consent involved negligence in the form of obtaining informed consent about the surgical procedure involved, with 4 cases awarding damages due to the fact that the plaintiff was not given sufficient information regarding the exact method and possible complications that may arise from surgery, and one case finding the defendant liable for obtaining informed consent from the patient's legal guardian but not the actual patient. Seven of the nine cases that ruled in favor of the plaintiff arose from primary/local clinics (Table 2).
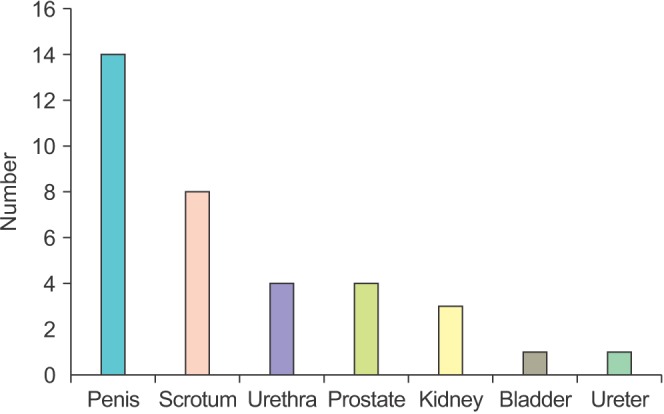
An analysis of the cases based on the sites of surgery revealed that the cases could be classified as being applicable to the following sites (in order of frequency): penis, scrotum, urethra, prostate, kidney, bladder, and ureter (Fig. 2). Some cases listed two or more sites of surgery; cases claiming misdiagnosis as the actionable violation were omitted from this classification.
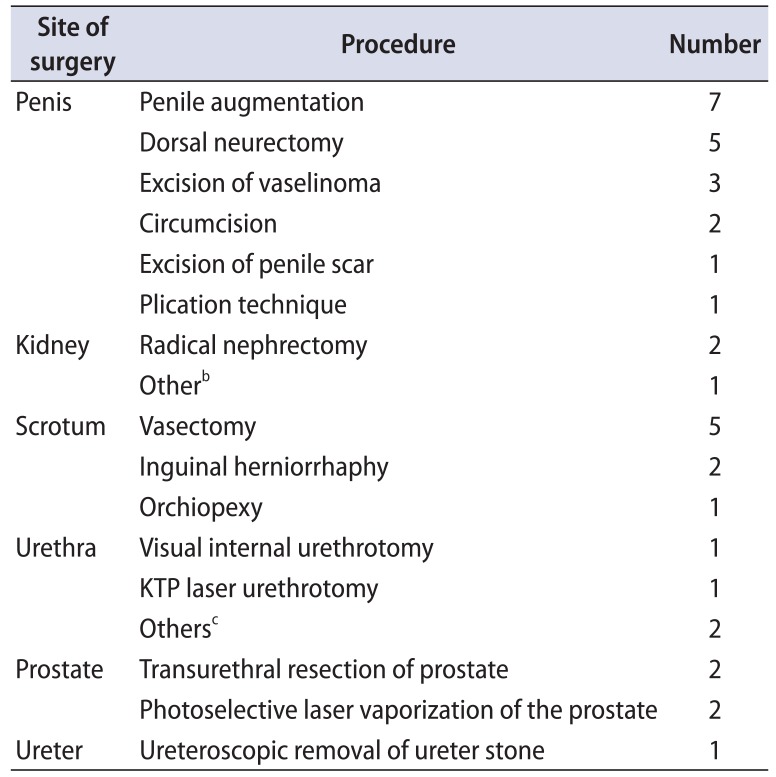
The types of surgery were further classified by their sites of surgery (Table 3). Cases that did not involve a surgical procedure and cases that involved only a cystoscopy were omitted from Table 3. Cases involving penile enlargement were most frequent with seven occurrences, followed by dorsal neurectomy and vasectomy with 5 cases each. All three surgical cases involving the kidneys were radical treatments for cancer.
DISCUSSION
This study aimed to determine the tendencies and frequently delivered verdicts in urology-related medical litigation by analyzing 34 unique cases involving urology. The results of this study can be used as baseline material for malpractice prevention research, while also providing useful information about malpractice for practitioners in the field of urology.
The average amount in damages paid out to plaintiffs in the cases analyzed here was 27,186,504 KRW. For comparison, plaintiffs in the field of plastic surgery receive an average of 22,682,450 KRW [10]. An average of 161,389,291 KRW is paid out to neonatal patients in court [9], and winning patients filing claims in orthopedics receive an average of 58,897,161 KRW [8]. Thus, claim amounts paid in urology tend to be at or below the averages in other medical specialties. In a malpractice suit, compensation is calculated on the basis of general damages (cost of treatment, convalescent care, etc.), special damages (lost earning capacity, etc.), and consolation money [19]. Malpractice concerning neonatal care and orthopedics show a tendency for permanent disability, which results in the patient being afforded substantial redress on the grounds of general damages [9], as well as a significant amount of money being paid out to cover the patient's lost earning capacity, resulting in higher thresholds of compensation. Nevertheless, damages awarded to a patient as a result of urology malpractice are in no way insignificant, and continuous effort must be expended to shield practitioners not only from the fiscal burdens of but also the mental stress that accumulates from preparing for, and the 3.8 years it takes on average for a practitioner to settle, a malpractice suit, as determined by this study.
In studies that analyzed malpractice trends in the United States, “improper performance of procedure” [182021] alongside “prostate cancer and transurethral prostate resection” were determined as leading causes of malpractice litigation [22]. A study based in the United Kingdom that analyzed resources published by the National Health Service Litigation Authority revealed that malpractice claims were centered around “nonoperative events,” “postoperative events,” and “intraoperative events” in terms of order of frequency [23]. The majority of court cases analyzed by this study revolved around events that occurred during surgery, and cases that held the medical practitioner as liable for breach of duty of care in court also stemmed from surgical events or (the lack of) postsurgical care. 32 of 43 cases brought forth to the Korea Medical Dispute Mediation and Arbitration Agency regarding urological care in 2016 claimed damages based on surgical events [24]. Differences in most of the claims were evident depending on the type of study, but litigation seems to more often than not arise as a byproduct of surgery owing to the fact that it in itself is an invasive medical procedure, with the possibility of error present at multiple levels of the process. Furthermore, surgery is thought to have a high tendency of birthing litigation because patients are not always fully conscious of the procedure they are about to undertake, and also because of the inherent dangers that accompany each procedure of the operation [2526].
Five of 34 cases charged the defendant with breach of duty of informed consent. The plaintiffs' claims as pertaining to the breach of duty of informed consent can be further broken down into three arguments. The first argument was that the patient did not receive the intended information even though sufficient information was provided by the physician. The second argument was that information was provided by the physician to the patient's family but not to the patient before the procedure. The third and most straightforward argument was that sufficient information was not provided to the patient. In the cases that argued the third claim, the plaintiff argued that the physician emphasized the positive impacts and results of the procedure instead of cautioning about the possible complications. This proved especially to be the case with litigation surrounding penile surgery, and parallels can be drawn to plastic and cosmetic surgery regarding this phenomenon [27].
It is therefore imperative to give consideration to patients' reasons for making the case about informed consent. Patients oftentimes will make the informed consent (or lack thereof) case because it is exceedingly difficult to prove in a court of law that the physician has neglected to perfectly and adequately explain the situation at hand to the patient [28]. On the other hand, this can be seen as a sign of dissatisfaction toward the quality of explanation provided by the medical personnel. It perhaps goes without saying that as far as the duty of informed consent goes for surgical procedures that involve a plastic element, providing adequate information and explanation regarding possible complications and side effects far outweighs any sort of emphasis on the potential positive effects of a successful procedure. Furthermore, patients should be given a tailored explanation of their individual situation and procedure in addition to the standard agreement or waiver they are required to sign prior to surgery.
The majority of claims (48.7%) involving urological surgery in Korea stemmed from penile surgery. Patients' reasons for filing suit following penile surgery included dissatisfaction from penile curvature resulting from postoperative complications, actual loss of penile length, scarring of the penile tissue, and glanular deformity. A review of nonurological literature revealed that 75% of claims against surgeons performing aesthetic procedures occurred as a result of dissatisfaction [29]. Patient dissatisfaction with postoperative results, and the physician's responsibility for ensuring the success of the surgery, was argued in court owing to the fact that penile surgery—among the few other types of surgery discussed in this study—tends to be neither urgent nor life-threatening, seldom placing the patient in great risk when delayed. In one particular case, a patient filed suit with the court citing great dissatisfaction with the result of his surgery, claiming that his genitalia became deformed resembling a sweet potato as a result of negligent penile augmentation surgery. Other patients have made similar claims to the court citing erectile dysfunction and difficulty in engaging in sexual activity as unwarranted adverse effects. In other cases, patients who have undergone nonpenile procedures such as vasectomy, transurethral resection of the prostate, or photoselective laser vaporization of the prostate have also made claims along the lines of decreased sexual function.
This study analyzed 34 cases, spanning a relatively brief period of 5 years. It is difficult to say whether this study adequately represents a complete picture of urology-related patient safety incidents, as the cases taken into account were limited to those registered with the court. It is difficult to identify each and every patient safety incident in relation to urological care with just the systems currently in place in Korea. However, with the enforcement of the Patient Safety Act in 2016, which launched the “System for Reporting and Learning of Patient Safety Accidents,“ and thanks in part to the Korea Medical Dispute Mediation and Arbitration Agency's continuous efforts in collecting data concerning arbitration of medical disputes, the need and opportunities for additional research in cooperation with these respective agencies will surely arise in the future. Other intangibles existed throughout the study due to the redaction of personal information in the case files provided by the court. Because the names of the medical institutions, the number of urology specialists on hand at each institution, the age of the patients, and other personally identifiable information was redacted from the received court records, some of the sensitive information relating to the cases in the study was ascertained through careful guesswork. This research retains significance, however, in the fact that it provides both quantitative and qualitative analysis of urology-related medical litigations despite these limitations.
CONCLUSIONS
All doctors inevitably experience medical dispute or malpractice litigation in one form or another at least once throughout their careers. Regardless of the outcome of said litigation, it is important that information regarding such disputes and lawsuits be made available to the medical community to help prevent further disputes and malpractice from occurring. This study analyzed the status quo and the unique characteristics surrounding urology-related litigation. The defendant was most frequently held liable for negligent acts performed during surgery, with the most frequently litigated type of surgery being performed on the penis. Common postoperative complications included erectile dysfunction and penile deformation.
An element of risk exists in every facet of medical treatment, and effective patient management is required to counteract such dangers. Keeping these factors in mind, continuous effort must be expended in the prevention of future accidents and litigation, alongside research into urology-related cases beyond 2010. Extensive cause analysis and recurrence prevention methods must also be researched to enhance overall patient safety and experience.
 XML Download
XML Download