

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The European Association of Urology 2014 guidelines for the treatment of nephrolithiasis recommend percutaneous nephrolithotomy (PCNL) as a first method of choice for stones >2 cm and shockwave lithotripsy (SWL) for stones <1 cm. For stones between 1 and 2 cm, either SWL, retrograde intrarenal surgery (RIRS), or PCNL can be used depending on the anatomical and stone characteristics. Nonetheless, recent technological advancements, brought about improvements in the design and performance of flexible ureteroscopes such as a reduced scope diameter, enhanced light diffusion, higher resolution, an extended visual field, and advances in distal tip deflection, have made it possible to manage nephrolithiasis with high stone burdens using RIRS instead of PCNL [12]. RIRS is also a treatment solution for patients with contraindications or who refuse to undergo PCNL [34]. Furthermore, PCNL is associated with various complications, including urinary extravasation, bleeding necessitating transfusion, and even life-threatening conditions, such as septicemia, and pleural and colonic injury, while RIRS minimizes these complications [56].
However, although there have been several previous reports that the stone-free rate of RIRS is comparable to that of PCNL [478], large renal stones are still treated extensively with PCNL because of its high stone clearance rate of approximately 95% [4]. Furthermore, RIRS suffers from a high retreatment rate and a relatively long operation time for patients with a high kidney stone burden. Therefore, it would be of great help to develop a practical method that increases stone clearance rate using this technique.
In this study, we analyzed the effect of preoperative SWL and investigated whether it improves the treatment outcomes of nephrolithiasis in terms of stone-free rate and number of repeated procedures after RIRS by comparing the results of patients who underwent SWL before surgery with those who did not.
Go to : 
MATERIALS AND METHODS
This study was performed with the approval and oversight of the Institutional Review Board at Asan Medical Center (approval number: 2013-0745). The data of 189 patients with nephrolithiasis who underwent RIRS from July 2007 to July 2014 at Asan Medical Center by a single surgeon were reviewed retrospectively. Patient age, body mass index (BMI), location, composition, density, size, number, and multiplicity of stone(s) were the variables reviewed. Stone size was estimated by measuring stone diameter in a computed tomography (CT) scan and recorded as a net size by adding the largest diameters of each stones, if stones were multiple. For group 1 patients, stone size was estimated before undergoing SWL. In addition, surgical parameters including operative time, hospital stay, and combined procedures such as balloon dilatation, endopyelotomy, and diverticular excision were also recorded.
1. Patient classification
Before the surgery, CT scans combined with abdominal plain films (kidney-ureter-bladder, KUB) were performed on all patients to examine the location and size of the stone(s). All patients were planned to undergo RIRS; however, the decision to perform SWL before the surgery was made jointly by the surgeon and the patient, while taking into consideration the size, number of stone(s) and/or economic status of the patients. SWL prior to RIRS was usually recommended to the patients who had stones larger than 1.5 cm. However, patients with multiple stones (more than 3) also underwent SWL, although their net size was smaller than 1.5 cm. In these patients, the shock wave was focused to a stone with the largest diameter. Therefore, patients were classified into 2 groups: Group 1 included patients who underwent SWL prior to RIRS (n=68), and group 2 included patients who underwent RIRS without preoperative SWL (n=121). Among them, there were 61 patients with stone(s) larger than 1.5 cm in group 2 patients. The SWL and RIRS were considered as one treatment protocol in group 1 patients with stones that are relatively large to perform RIRS only. Operative times, number of repeated procedures, and stone-free rates of the 2 groups were compared. A stonefree state was defined as no visible residual stones on a CT scan after a single RIRS.
2. Treatment procedure
All patients in group 1 underwent single session of preoperative SWL, carried out by a single operator using a fourth generation electroconductive lithotripter (Sonolith Vision, EDAP TMS, Vaulx-en-Velin, France) 2 weeks before RIRS. In this group of patients, CT scan and/or KUB was checked to examine the stone(s) after SWL and before surgery. Presence of remained stone(s) was confirmed by CT scans in all group 1 patients. Representative CT scan images before and after SWL, and after RIRS is shown in the Fig. 1. For RIRS, a safety hydrophilic guide wire was placed into the renal pelvis by use of 8/8.9-Fr semirigid ureteroscopy af ter induction of general anesthesia. Retrograde pyelography by fluoroscopy with contrast dye was performed to examine the size and location of the stone(s). A 2-way actively deflectable (270°/270°) flexible ureteroscope (Wolf Cobra, Knittlingen, Germany or Flex-X2, Karl Storz, Tuttlingen, Germany) with a ureteral access sheath was used to perform RIRS in all patients. Incision of diverticular neck (if calyceal diverticuli were present) and fragmentation of stone(s) was performed with 200-µm diameter holmium: YAG laser fibers at an energy level of 0.6–1.2 J and at a rate of 5–10 Hz. Fragmented stones were retrieved with a stone basket or removed by irrigation. At the end of the procedure, the entire collecting system was inspected to confirm stone clearance. A JJ ureteral stent was not inserted before the surgery and/or SWL, it was routinely positioned in all patients immediately after the surgery only, and was removed 2 weeks after in an outpatient clinic. All of the procedures were performed by a single surgeon. A postoperative follow-up CT scan was performed 1–2 month(s) after surgery to examine for the presence of residual stones.

3. Statistical analysis
For the adjustment of imbalances in preoperative characteristics that may influence stone-free rate among 2 patient groups, propensity scores were calculated for each subject using multivariate logistic regression based upon stone size, number and location. Patients in the 2 groups were matched at a 1:1 ratio based on propensity scores. The Student t-test and Pearson chi-square test were used to compare the mean values for the continuous and categorical variables, respectively. Univariate and multivariate analysis was performed with logistic regression to investigate factors predicting a stone-free state. All statistical analyses were performed with IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA), all tests were 2-sided, and statistical significance was considered at p-values less than 0.05.
Go to :
RESULTS
Patients in both groups were matched 1:1 with respect to the size, number, and location of stone(s) which left 57 patients in each group. Before matching, the sizes of stones in group 1 patients were significantly larger than those in group 2 patients (1.7 cm vs. 1.1 cm, respectively, p<0.001), while other stone characteristics, including number, location, density, composition, and multiplicity of stones, did not show any significant differences between the 2 groups. There was no such patient who underwent unnecessary surgery due to prior SWL in group 1 patients because of relatively large stone size. The mean value of stone size in group 1 patients after SWL was 1.1±0.7 cm. The baseline demographics of the patients in the 2 groups showed no significant differences in terms of age, BMI, and sex, or in stone characteristics after matching (Table 1).
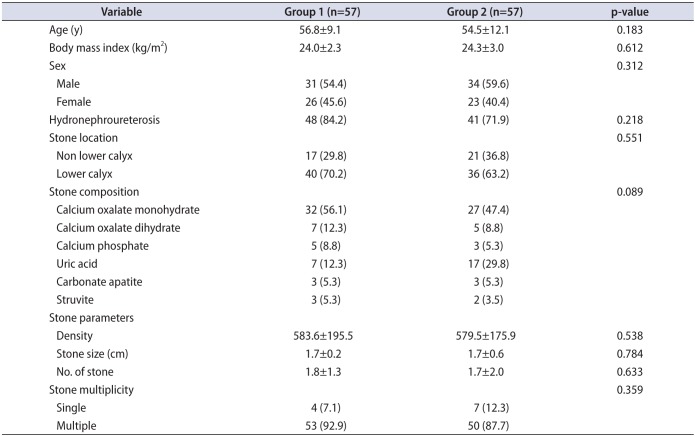
Table 1
Preoperative patient and stone characteristics after propensity score matching
![]()
The overall mean operation time was 70.5±24.6 minutes and hospital stay was 2.7±1.9 days. There were no notable complications associated with SWL in group 1 patients. Complications related to surgery occurred in three patients in the 2 groups, but these were minor (transient postoperative fever; Clavien-Dindo grade I [9]). Among the 21 patients who underwent a repeated ureteroscopy, no patient was subjected to the procedure three times or more. The operative time, length of hospital stay, number and types of combined procedures during RIRS, and complication rates did not show any differences between the 2 groups. However, stone-free rates after a single RIRS were significantly higher in group 1 patients than in group 2 patients (89.4% vs. 73.6%, respectively, p=0.039), and the number of patients requiring repeated ureteroscopic lithotomy (including semirigid and/or flexible) was lower in group 1 patients (10.6% vs. 26.4%, respectively, p=0.035). The perioperative and postoperative data are compared in Table 2.
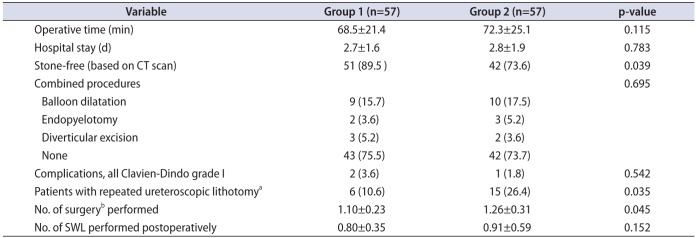
Table 2
Comparison of perioperative and postoperative outcomes between the groups
Values are presented as mean±standard deviation or number (%).
Group 1, patients who underwent SWL prior to RIRS; group 2, patients who underwent RIRS without preoperative SWL; SWL, shockwave lithotripsy; RIRS, retrograde intrarenal surgery; CT, computed tomography.
a:Includes semirigid and/or flexible ureteroscopy. b:Included retrograde intrarenal surgery and ureteroscopic lithotomy.
![]()
Among the various patient and stone characteristics in the entire patient cohort (including groups 1 and 2, n=114), presence of hydronephroureterosis, location, density, and size of stone(s), and preoperative SWL were significant factors predicting a stone-free state in univariate analysis (Table 3). However, in multivariate analysis, Non lower calyceal stone location, stone density, stone size and preoperative SWL were independent predictors of a stone-free state, while hydronephroureterosis was not a significant factor.
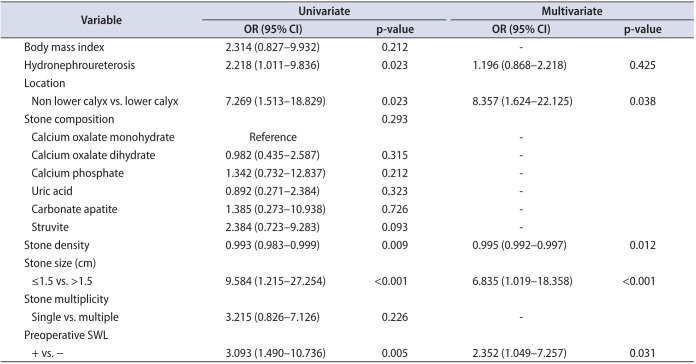
Table 3
Univariate and multivariate analysis of factors predicting stone-free state
![]()
Go to :
DISCUSSION
Urinary tract stone disease causes not only troublesome symptoms such as pain, but also may lead to chronic kidney disease and even end-stage renal disease if left untreated, and its incidence in industrialized countries has increased with the rise in living standards [10]. Therefore, careful monitoring and appropriate treatment are essential in patients with kidney stone disease.
Current guidelines for nephrolithiasis clearly recommend PCNL as a first line of treatment for stones larger than 2 cm in diameter because of the high efficacy of this technique. For stones smaller than 2 cm and larger than 1 cm, both RIRS and PCNL are treatment options. Most previous studies reported PCNL stone clearance rates as high as 90% to 95% [1112]. However, despite technological advancements, PCNL still has significant rate of serious complications [6913]. The estimated rates of complications were 0.9% to 4.7% for septicemia, 0.6% to 1.4% for severe bleeding requiring transfusion, 2.3% to 3.1% for pleural injury, and 0.2% to 0.8% for colonic injury [14]. On the other hand, improvements in endoscopic equipment and techniques, such as in flexible ureteroscopes and laser lithotripsy, have increased the efficacy of RIRS for the treatment of relatively large stones in difficult locations. Advances in distal tip movements and increases in the durability of flexible ureteroscopes have made it possible to access stones located at the lower pole [15]. Along with this, RIRS is less invasive and has lower complication rates than PCNL [131617]. In addition, RIRS is considered to be a day-care outpatient procedure or a procedure that at most requires a short hospital stay. Therefore, it is increasingly considered an alternative treatment option to PCNL, especially for stones in the size range 1–2 cm [218]. However, the reported stone clearance rate of RIRS is variable and ranges from 50% to 94.2% [192021]. Although there were some reports of comparable results between RIRS and PCNL [413], other reports comparing the outcomes of RIRS and PCNL have shown that RIRS is inferior to PCNL in terms of stone clearance and retreatment rates [2223]. Chung et al. [8] compared the treatment outcomes of 15 and 12 patients with 1- to 2-cm-sized renal stones who underwent PCNL and RIRS, respectively. The stone-free rates were 87% for patients treated with PCNL and 67% for those treated with RIRS. The lower stone clearance rate of RIRS was mostly attributed to the large size and lower pole location of stones [24]. Therefore, increasing the treatment success rate of RIRS is considered worthwhile because it would increase its use in clinical practice, resulting in lower complication and morbidity rates than those of PCNL.
We postulated that performing SWL before surgery would help induce stone fragmentation and reduce stone burden, thereby shortening the operative time, decreasing the need for repeated procedures, and ultimately enhancing the stone-free rate. In our study, performing SWL actually decreased mean stone size in group 1 patients from 1.7±0.2 to 1.1±0.7 cm. Our data also showed that the average operative time was 70.5 minutes, which was shorter than those of previously reported series [252627]. However, although the mean operative time in group 1 patients was slightly shorter than that of group 2 patients, the difference failed to reach statistical significance. We attribute the better stonefree rate in group 1 patients to the prior fragmentation of the stones accomplished by SWL before surgery, which would have resulted in a reduction in the amount of effort required during the subsequent RIRS procedure. Indeed, the stone-free rate was higher and the number of patients who underwent a repeat ureteroscopy afterwards was smaller in group 1 patients. One of the most important disadvantages of RIRS is the requirement for a second procedure. The reported success rate of RIRS has reached 77%–93% but this includes additional sessions for renal stones larger than 2 cm [4]. According to our results, preoperative SWL should be encouraged to reduce the need for supplementary procedures. Furthermore, the average stone clearance rate of the total patient cohort in this study after a single session of RIRS was relatively high at 81.5%, which may be due to the same reason for short operative time. Thus, our novel method may be an effective and also safe way of treating patients with nephrolithiasis larger than 1.5 cm because it results in relatively high success rate as well as very low complication rates.
Major drawbacks of this study are first, its retrospective design and lack of a randomization process. Because the patients were divided into 2 groups according to stone size, number, and patient and/or surgeon preference without randomization, a potential selection bias cannot be strictly ruled out. To overcome this, we performed 1:1 matching using a propensity scoring system for the adjustment of stone size, number, and location. As a result, the stone characteristics of each group of patients including location, composition, size and number of stones did not show any statistical difference. Second, cost implications between the 2 groups are not included in this study. However, to the best of our knowledge, our study is the first report to demonstrate the efficacy of performing SWL prior to RIRS. We are planning to perform a randomized controlled study to confirm the positive effect of this novel procedure in patients with certain stone size (e.g., 1–2 cm) in the near future.
Go to :
CONCLUSIONS
In conclusion, performing SWL before RIRS may be a safe and effective way to facilitate stone elimination during surgery and increase the stone-free rate. In addition, it may reduce the necessity for repeated procedures and therefore expand the indication of RIRS. Further prospective randomized studies are required to confirm these outcomes.
Go to :
 XML Download
XML Download