

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic prostatitis (CP)/chronic pelvic pain syndrome (CPPS) is a very common prostatic disease in those younger than 50 years and constitutes 8%–14% of urology clinic visits [1]. The impact of CP on the patients' quality of life (QoL) is severe due to its typical chronic pelvic pain and accompanying voiding symptoms [2].
Numerous studies exist regarding CP/CPPS in adult patients; however, reports on adolescent CP/CPPS are rare, possibly due to the low incidence of CP/CPPS in adolescence.
A recent community study showed a 13.3% prevalence of CP-like symptoms in adolescent males [3]. Although the prevalence seen in previous studies is somewhat lower than in this study, prevalences as high as 2.0%–8.3% were seen [45].
Community prevalence is different from that seen in urology department patients; CP-like symptoms could include many other disorders besides CP/CPPS. The possibility of underestimation of CP/CPPS during adolescence has to be considered.
During puberty, the reproductive function of the prostate becomes active; prostatic secretions comprise a major portion of the semen. The prostate grows rapidly during adolescence due to the pubertal surge in serum testosterone levels [6].
Inflammation during this period of rapid growth has a harmful effect on the normal physiological process of the prostate; this could also create problems in adolescence, which is known as a critical period for mental, social, and emotional development [7]. It is therefore necessary to study adolescent CP/CPPS, especially in comparison with adult CP/CPPS.
One report about CP/CPPS during puberty showed predominant pelvic floor disorder and that biofeedback was effective for controlling symptoms in adolescents [8]. They reported that majority of pubertal CP/CPPS cases were classified into category III-B. Additionally, voiding disorder was the dominant symptom; this is different from the paindominant clinical situations and the even distribution of category III-A and III-B in adult CP/CPPS cases.
We therefore compared the clinical characteristics of adolescent CP/CPPS patients to those of young adult patients to investigate these issues.
MATERIALS AND METHODS
A prospective study plan was tried initially, but we changed it to a retrospective one due to the very small number of the patients who were finally diagnosed as adolescent CP/CPPS in the outpatient urology department. We reviewed charts of patients with chronic pelvic pain aged <20 years who were finally diagnosed as having CP/CPPS from August 2005 to April 2012. The Institutional Review Board of Inje University Ilsan Paik Hospital approved this retrospective study (approval number: ISPAIK 2017-01-013). The inclusion criteria were: patients with at least 3 months duration of chronic pelvic pain symptoms and no other identifiable urologic anomalies or diseases. In all patients, urinalysis and urine culture was performed and other abnormalities were excluded. To rule out urinary tract anomaly, intravenous urography and ultrasonography of the kidney and scrotum was performed. All patients were tested for sexually transmitted infection (STI) using serum tests for syphilis, chlamydia, human immunodeficiency virus, and herpes virus. In some patients, polymerase chain reaction tests for Trichomonas vaginalis, Mycoplasma hominis, Mycoplasma genitalium, Chlamydia trachomatis, Nisseria gonorrhea, and Ureaplasma urealyticum were performed; it was confirmed that no patient with STI was included in the study. After excluding all other possible diagnoses, the patients were finally diagnosed as CP/CPPS. A complete medical history and thorough physical examination were performed. The national institute of health-chronic prostatitis symptoms index (NIH-CPSI) questionnaire, expressed prostatic secretion (EPS) or semen analysis, transrectal prostate ultrasonography (TRUS) and prostatespecific antigen (PSA) were performed. Twenty patients were eligible for enrollment in the study. The control group comprised 120 CP/CPPS patients aged 20–39 years who visited outpatient department during the same period. This group was created to rule out the effects of benign prostatic hypertrophy. Clinical case history, thorough physical examination, urinalysis, NIH-CPSI questionnaire, EPS or semen analysis, TRUS, and PSA testing were performed in the control group. Based on the EPS or semen analysis results, patients were divided into category III-A or III-B CP/CPPS. The clinical parameters of the adolescent CP/CPPS group were compared with those of the young adult group. Results were statistically analyzed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). The independent t-test was used, and a p-value less than 0.05 was regarded as significant.
RESULTS
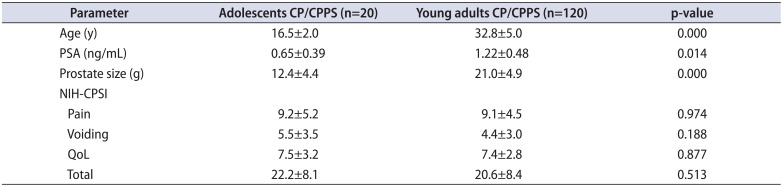
The mean patient age was 16.5±2.0 years (range, 12–19 years) and 32.8±5.0 years (range, 20–39 years) in the adolescent and young adult CP/CPPS groups, respectively. In the adolescent group, there was a history of sexual contact in 2 patients (10%); they were categorized as inflammatory type (category III-A). The most common pain site was the testes, seen in 7 patients (35%). The inflammatory CP/CPPS (category III-A) had 9 patients (45%) and the noninflammatory CP/CPPS (category III-B) had 11 patients (55%). In the young adult group, category III-A and III-B had 67 (56%) and 53 patients (44%), respectively.
The PSA was 0.65±0.39 ng/mL (range, 0.20–1.30 ng/mL) and 1.22±0.48 ng/dL (range, 0.25–2.01 ng/mL) in the adolescent and young adult groups, respectively (p=0.014). The prostate size was 12.4±4.4 g (range, 3.2–17.3 g) and 21.0±4.9 g (range, 12.0–33.0 g) in the adolescent and young adult patients, respectively (p=0.000).
The NIH-CPSI scores in the adolescent group were 9.2±5.2 (range, 0–16), 5.5±3.5 (range, 0–10), 7.5±3.2 (range, 3–12), and 22.2±8.1 (range, 7–38) for pain, voiding, QoL domains, and total score, respectively. The adolescent group showed a tendency to have relatively higher voiding symptom domain scores. However, this difference was not statistically significant. Other domain scores did not show any significant difference (p>0.05) (Table 1).
DISCUSSION
There is a discrepancy between the high prevalence of CP-like symptoms seen in community studies [345] and the small number of adolescent CP/CPPS patients seen in urology outpatient departments.
This could be due to the fact that community survey data could include cases of urinary or STI, which could present CP-like symptoms. In fact, after removing the question items related to such symptoms, the prevalence of CP-like symptoms decreased from 13.3% to 9% for mild symptoms and from 5.4% to 2.4% for moderate to severe symptoms [3].
Besides urinary or STI, other conditions could also mimic CP/CPPS and increase the prevalence of CP-like symptoms.
However, this cannot exclude the possibility of underestimation of adolescent CP/CPPS, as the incidence is not as rare as was thought to be previously. Urology department visits due to CP/CPPS are very low in adolescents compared to those in the adult population. However, this could also be due to ignorance regarding the meaning of these symptoms.
CP/CPPS is a bothersome disease and usually difficult to manage. Patients often expect to be disease-free after short-term treatment, like in simple UTIs. Patients often need to be educated regarding the necessity of long-term treatment and the fact that the chronic recurrent nature of the symptoms can reduce the patients' QoL [910]. CP/CPPS is known to be correlated with psychiatric or psychological problems, although the causality between the 2 conditions is unknown. The psychological status could affect the QoL in CP/CPPS patients [11] and vice versa. Adolescence is marked by rapid physical and mental changes; adolescents are psychologically vulnerable even in a healthy state [7]. Therefore, the psychological burden caused by chronic CP/CPPS could be much more severe than that in adult CP/CPPS patients.
In this study, the total NIH-CPSI scores in the adolescent group were high (22.2), revealing that CP/CPPS is equally devastating for adolescents. All the domain scores were evenly distributed in both age groups. A relatively higher voiding symptom domains score was noted in adolescents; although this difference was not statistically significant. We believe that this might be due to the small number of adolescent patients in our study. Other studies dealing with adolescent CP/CPPS patients have also reported a dominance of voiding problems; these studies postulated that pelvic floor disorders were also a factor in the etiology of adolescent CP/CPPS and that these symptoms are improved by biofeedback therapy targeting the pelvic floor [8]. However, in a community survey of CP-like symptoms during adolescence, the tendency of prominent voiding symptoms was not found [35].
The results of this study revealed no tendency or difference in the pain score and QoL score between the adolescent and young adult groups. The pain severity itself seems to be similar in both groups, but due to the previously mentioned vulnerability in adolescents, the psychological impact could be higher in adolescent CP/CPPS patients. This could be the reason why a multifactorial approach involving psychological assessment seems warranted in the analysis of adolescent CP/CPPS.
Many diseases presenting with chronic symptoms exhibit a discrepancy between a relatively high prevalence in community surveys and a lower number of hospital visits. In the case of adolescent CP/CPPS patients, this could be due to the specific issues seen in adolescence as well as unawareness or misunderstandings regarding CP/CPPS.
In the subclassification of CPPS, the proportion of noninflammatory CPPS (category III-B) was higher in the adolescent group (55%) than in the young adult group (44%). Although classification of this condition into inflammatory or noninflammatory types is difficult, and a change of class during follow-ups or after repeated prostatic massage is not rare, the proportion of non-inflammatory CP/CPPS is usually higher or at least the same [12]. In this study, the adolescent group showed a higher proportion of the noninflammatory class compared with the young adult group, which is consistent with results of other studies. Li et al. [8] reported category III-B as the dominant subtype in CP/CPPS during puberty; voiding symptoms were predominant in their study as well. When considering the very low number of adolescent CP/CPPS visits to the urology department, it is difficult to assess the true subclass distribution.
This study has several limitations. First, it is a retrospective study and psychodynamic assessment was not done, which we realized was important only after the data collected for this study was analyzed. The second limitation is the small number of patients. We could find only 20 patients during the study period of 7 years; again, this represents the rarity of hospital visits in adolescent CP/CPPS patients.
CONCLUSIONS
As seen in adult patients, adolescent CP/CPPS is devastating and has a significant negative impact on the QoL. Compared with young adult patients, adolescent CP/CPPS patients aged <20 years showed a tendency to have relatively high voiding symptom scores, but no differences were found in terms of other urologic clinical parameters. Further studies on adolescent CP/CPPS are required for the clarification of this uncommon but important disorder.
 XML Download
XML Download