

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Renal cell carcinoma (RCC) represents 4% of all new diagnosed malignancies, with over 62,000 new cases expected in 2016 [1]. Many of these newly diagnosed malignancies include incidental, small, and localized lesions, attributable to the widespread use of abdominal imaging modalities [2]. Surgical management with partial nephrectomy (PN) is the standard approach for most small renal lesions concerning for RCC, with very favorable outcomes [34]. Imaging modalities are highly useful for stratifying patients at risk for renal malignancy; however, upwards of 30% of excised lesions ultimately show benign pathology [5]. While there are certainly indications for excision of benign tumors, these lesions are often unnecessarily surgically excised due to ambiguity of diagnosis and risk of malignancy. Distinguishing oncocytoma or lipid-poor angiomyolipoma (AML) from RCC is difficult [678], and it is clear that better preoperative risk models are needed to prevent unnecessary surgeries for benign lesions.
AMLs are benign kidney lesions that are normally distinguished from RCC on imaging due to fat content. RCC rarely contains macroscopic adiposity, while close to 5% of AMLs do not exhibit macroscopic fat upon standard imaging and are classified as “lipid-poor AML” [78]. Previous studies have used imaging characteristics to help with distinguishing lipid-poor AML from RCC [910111213141516]. Despite this progress, detection of lipid-poor AML remains difficult, and directly conflicting results exist in the literature for some imaging findings [1516]. While there is a noted association of AML with age and sex [17], there are few models that accurately predict lipid-poor AML using preoperative patient characteristics. Therefore, the objective of this study was to use clinical variables to create a simple model for predicting lipid-poor AML in patients with small renal masses presumed to be RCC from preoperative imaging.
MATERIALS AND METHODS
1. Patient cohort
The Washington University Institutional Review Board approved the prospective collection of patient data used in this study (approval number: 201304085). Using a consented, de-identified, prospectively maintained database, all patients undergoing PN between 2007 and 2015 were retrospectively identified. Only patients with preoperative imaging suspicious for malignancy were included, and this was defined as solid enhancing masses or complicated renal cysts classified as Bosniak category III or IV [18]. Patient were excluded if given a previous diagnosis of von Hippel-Landau syndrome, tuberous sclerosis, or Birt-Hogg-Dubé syndrome, or if more than one renal mass was resected or preoperative imaging was suspicious for benign lesions. The final cohort of patients underwent a single PN for a single renal lesion with curative intent for presumed RCC.
2. Surgical technique
Surgical approach was impacted by the following factors: patient habitus, tumor location, history of abdominal surgery, and surgeon and patient preference. A transperitoneal approach was used for laparoscopic operations with clamping of the renal vessels [19]. Open PN was used for larger endophytic tumors and was based on surgeon preference. Robotic-assisted PN (RAPN) operations were performed with a retroperitoneal or transperitoneal approach [20]. Off-clamp technique was chosen based on tumor location, patient characteristics, and surgeon preference [21].
3. Data collection
Staff data managers and physicians prospectively collected patient demographics, perioperative outcomes, and tumor characteristics. AML was considered “lipid-poor” and was included in this study if adiposity was not observed on preoperative imaging and if the lesion was considered suspicious for malignancy. Preoperative computed tomography (CT) or magnetic resonance imaging (MRI) was interpreted by fellowship-trained genitourinary radiologists before the time of surgery, and genitourinary pathologists were responsible for making the final diagnosis.
4. Statistical analysis
Chi-square analysis, Fisher exact test, or Mann-Whitney U-test were used to evaluate the association of preoperative variables with lipid-poor AML. Logistic regression was used for multivariable modeling of predictors of lipid-poor AML using the following variables: sex, age at surgery, preoperative hemoglobin, history of hypertension, and tumor size. Point values for the final model were created by normalization of odds ratios to the lowest value from multivariate analysis, where the lowest odds ratio was assigned a point value of one. All analysis was performed using R v3.1.3 (R Foundation for Statistical Computing, Vienna, Austria), and a 2-tailed p-value <0.05 was considered significant in all analyses.
RESULTS
A total of 730 patients underwent PN at our institution between 2007–2015 for renal masses ≤4 cm, including 110 patients (15.1%) with benign pathology upon final diagnosis (Table 1). Of these 110 patients, 35 patients (31.8%) were diagnosed with AML. All cases of AML were retrospectively confirmed to be lipid-poor AML by evaluation of surgical pathology reports.
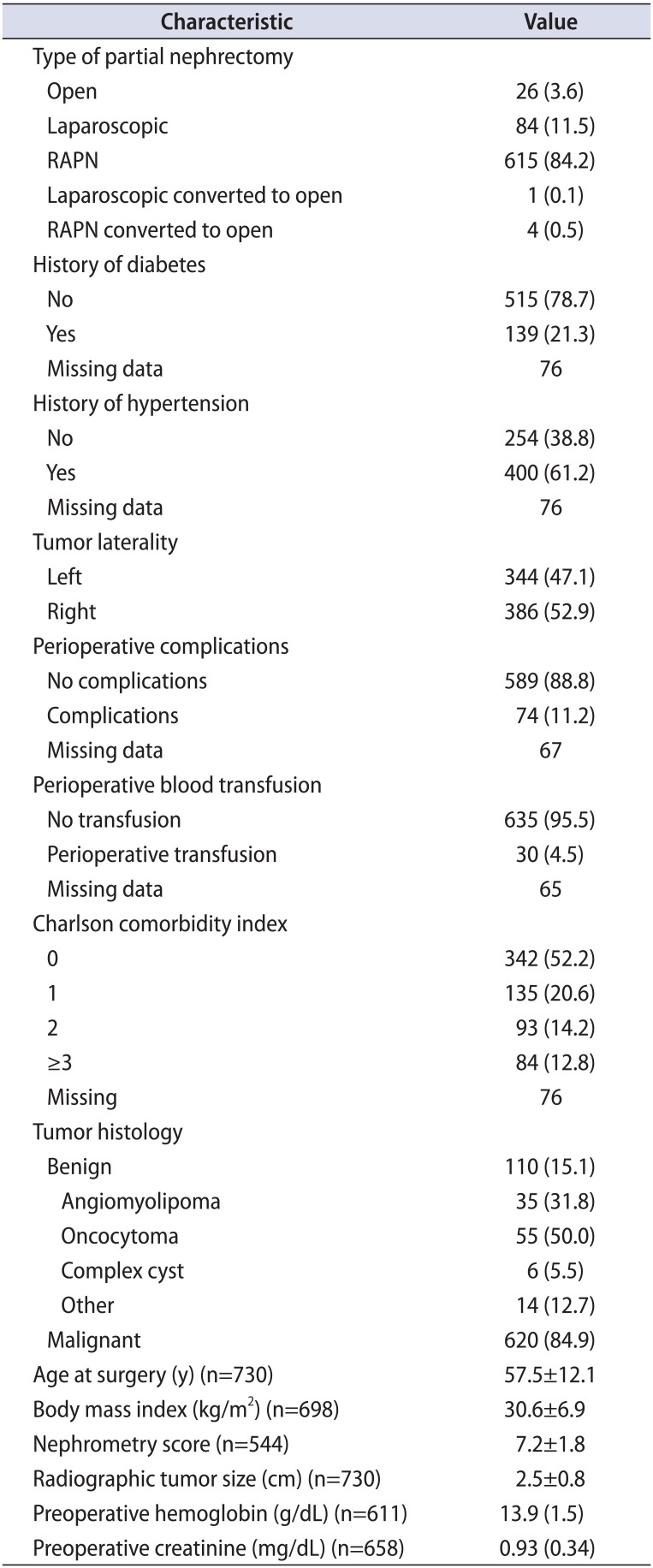
Table 1
Demographics of patients undergoing partial nephrectomy for ≤4-cm lesions presumed to be RCC from preoperative imaging
![]()
Differences in patient characteristics between patients with RCC (n=620) and lipid-poor AML (n=35) were then investigated (Supplementary Table 1). Compared to patients with RCC, patients with AML were significantly younger (p=0.01), more likely to be female (p<0.001), had smaller tumors (p<0.001) and lower nephrometry (p=0.003) scores, were less likely to have hypertension (p=0.02), and had lower preoperative creatinine (p<0.001) and hemoglobin (p=0.04). Within individual components of the nephrometry score, tumors in lipid-poor AML patients were located further from the collecting system (low N) (p=0.02) and were more likely to be highly exophytic (low E) (p=0.001). There was no significant difference in body mass index, comorbidity status, tumor laterality, anterior/posterior tumor location, tumor location relative to polar lines, or presence of diabetes mellitus between patients with RCC and lipid-poor AML.
A multivariable model was constructed to compare features and demographics of ≤4-cm masses in AML and RCC patients (Table 2). The following features independently predicted AML: female sex (odds ratio, 6.89; 95% confidence interval, 2.35–20.92; p<0.001), age <56 years (2.84; 1.21–6.66; p=0.02), and tumor size <2 cm (5.87; 2.70–12.77; p<0.001).
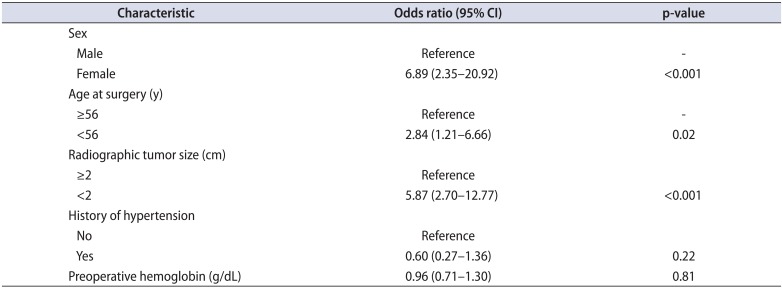
Table 2
Multivariable analysis of preoperative predictors of angiomyolipoma vs. malignant histology in renal masses ≤4 cm
![]()
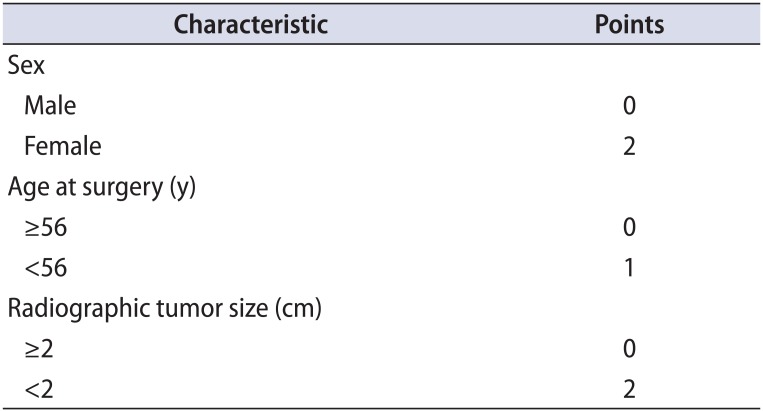
We hypothesized that these features could be used to create a simple model to distinguish lipid-poor AML from RCC in patients with ≤4-cm renal masses (Table 3). Sex, age, and tumor size were used to construct the BEnign Angiomyolipoma Renal Susceptibility (BEARS) index, where the following point values were assigned for each particular risk factor: female sex (2 points), age <56 (1 point), and tumor size <2 cm (2 points). Within the study population, the BEARS index distinguished AML from RCC lesions with an area under the curve of 0.84 (p<0.0001) (Fig. 1). Probability estimates for predicting lipid-poor AML were generated based of BEARS index values (Supplementary Table 2).

Fig. 1
Receiver operating characteristic analysis of the ability of the BEnign Angiomyolipoma Renal Susceptibility (BEARS) index to differentiate lipid-poor angiomyolipoma and renal cell carcinoma in renal masses ≤4 cm. The BEARS index was calculated for each patient using sex, tumor size, and age at surgery. The index significantly predicted lipid-poor angiomyolipoma histology after partial nephrectomy (area under the curve [AUC]=0.84; p<0.0001).
![]()
DISCUSSION
The ability to distinguish benign from malignant renal lesions preoperatively is important for preventing unnecessary surgeries, undue morbidity, and excessive medical costs. However, benign lesions such as oncocytoma and lipid-poor AML cannot be reliably distinguished from RCC with standard imaging modalities [678]. Previous studies have investigated whether preoperative characteristics can predict benign histology after PN [2223]. Both Jeon et al. [23] and Fujita et al. [22] reported that female sex and age at surgery were independently predictive of benign lesions. Further, Jeon et al. [23] found that earlier year of surgery was associated with benignity, while Fujita et al. [22] observed a relationship of exophyticity with benign lesions. Interestingly, AML was highly represented in the cohorts from Jeon et al. [23] (43.2% AML) and Fujita et al. [22] (41.6% AML), which led us to hypothesize that the high AML representation was driving the predictive factors observed in these studies. This was further corroborated by our institutional experience, where sex and age did not predict benignity in a cohort of patients with higher oncocytoma representation (51.2%) and a lower proportion of AML (28.6%).
There is a known association of AML with middle-aged females [17], and in this study, both age and sex were strong predictors of lipid-poor AML in multivariate analysis, suggesting that these variables also apply to lipid-poor AML in addition to lipid-rich AML. Interestingly, we limited our cohort to patients with tumors ≤4 cm given the small size of most lipid-poor AMLs and difficulty in management of small renal masses [24]. Despite limiting our cohort to tumors ≤4 cm, tumor size was the second strongest predictor of AML in our patients, with an odds ratio of 5.87. By combining these variables to create the BEARS index, we were able to accurately distinguish lipid-poor AML from RCC with an AUC of 0.84. From these data, we conclude that younger female patients with renal tumors <2 cm are at high risk of having AML instead of RCC, and alternative management decisions, including possible biopsy, should be considered before extirpative therapy in these patients.
Previously, multiple studies have used imaging features in attempt to distinguish lipid-poor AML from RCC and other lesions [910111213141516]. Authors have found myriad predictive factors of lipid-poor AML, including high attenuation on unenhanced CT [142526], a low T2-weighted signal intensity on MRI [1112], and homogenous tumor enhancement on contrast CT [1314], among other factors. However, it has been historically challenging to reliably distinguish lipid-poor AML from RCC based upon radiographic data alone [678]. There is difficulty in replicating results from previous studies, as conflicting results exist in the literature for some imaging results [1516]. Further, most patients receive either MRI or CT imaging, but not both modalities; therefore, imaging studies where only one modality is used limits applicability to all patients. Herein, we introduce the BEARS index, a simple model to predict the likelihood of AML in patients with small renal masses ≤4 cm. This model was highly accurate in classifying patients with masses ≤4 cm as lipid-poor AML, and the included components are readily available at most institutions, substantially increasing the potential clinical applicability. Through risk stratification and preoperative counseling, simple models such as the BEARS index may significantly reduce the number of patients undergoing unnecessary PN for benign lesions.
Limitations of the current study are inherently attributable to the retrospective design. There was variability in imaging protocols used for renal mass characterization. The number of patients with lipid-poor AML is a limitation, though few studies exist with larger cohorts. The BEARS index was created from and validated in the same cohort of patients; while the index was accurate in classifying AML in this set of patients, the instrument still needs to be validated externally.

 XML Download
XML Download