

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Penile carcinoma is an aggressive urologic malignancy in which the most significant prognostic variable is the presence and extent of lymph node involvement [1234]. Therefore, considerable interest has focused on the inguinal lymph node dissection (ILND) which provides valuable pathologic staging [567], guides adjuvant therapy [8], and offers therapeutic benefit [9]. Multiple studies, as reflected in current TNM staging for penile cancer [10], have shown that number of positive lymph node (LN) predicts recurrence-free survival (RFS) and overall survival (OS) [71112]. However, these studies do not account for the extent of ILND, masking the true extent of lymph node involvement. Recent literature has shown lymph node density (LND), defined by percentage of positive LN, is a superior prognostic tool for oncological outcomes after ILND by accounting for both extent of dissection and nodal disease burden [13141516].
While previous literature has demonstrated a prognostic benefit for LND, the studies are relatively few in number. Furthermore, there is considerable disagreement in the LND cutoff used to differentiate poor versus favorable survivability, ranging from 6.7% to 33% [131416]. The discordance may be explained by a significant variation in the total number of lymph nodes removed in previous studies, inclusion of patients with limited lymph node dissections, as well as varying statistical rationales used to calculate the cutoff. The wide range of nodes removed is also related to the inclusion of patients who simultaneously underwent pelvic lymph node dissection in patient cohorts, skewing the LND calculation.
The objective of this study was to validate the use of LND as a predictor of RFS and OS after ILND. We compare our results and analysis with the literature in an effort to reconcile the variation in cutoff LND and identify how different patient populations and statistical rationales have affected the results.
MATERIALS AND METHODS
Our institutional penile cancer database was queried for patients who underwent ILND from 1988 to 2012. Demographic and pathologic characteristics were analyzed to determine impact on RFS and OS. LND or the percent of positive LN out of total LN was calculated as a categorical variable at varying thresholds of 10%, 15%, and 20%. In patients who underwent simultaneous pelvic lymph dissection, positive pelvic lymph nodes were accounted for in the multivariable model, but were not included in calculations for lymph node yield or LND. from analysis. Patients underwent bilateral modified templates in all cases. In patients with nonpalpable nodes, a superficial dissection above the fascia lata was performed. In cases with palpable adenopathy or suspicious nodes encountered during superficial dissection, a deep dissection was performed. Pelvic lymphadenectomy was performed in patients with positive deep inguinal lymph nodes or with enlarged pelvic lymph nodes on cross sectional imaging. All nodal and fibroadipose tissue was completely embedded prior to pathologist analysis. At the time of primary tumor and lymph node dissection, specimens were reviewed both by general surgical pathologists and at a daily consensus surgical pathology conference attended by at least one senior urological pathologist for issues relating to grade, stage and margins.
Descriptive statistics were used to summarize patient characteristics and pathologic features. Continuous variables were compared with the Wilcoxon rank-sum or Kruskal-Wallis tests and categorical variables with the chi-square test.
Survival analysis was performed using the Kaplan-Meier method to determine RFS. The log rank test was used to compare survival curves. OS was calculated from the date of surgery to death from any cause or last follow-up. RFS was calculated from the date of surgery to local or distant recurrence or death from cancer. All patients were prescribed a follow-up regimen based on the National Comprehensive Cancer Network guidelines with physical exam every 3–6 months, depending on nodal stage. Cancer and vital status were determined by both clinical follow-up at Johns Hopkins University and by a query of the Social Security Death Index. Multivariable Cox proportional hazard models including primary tumor stage, patient age, medical comorbidities, pelvic lymph node status and total number of positive LN were constructed to adjust for potential confounding. Finally, Harrell's c index for OS and RFS were calculated for both LND and total number of positive nodes to determine which variable is the superior predictor of RFS and OS. All statistical analysis was performed with Stata 13 (StataCorp., College Station, TX, USA). Two-sided p values <0.05 were considered significant.
RESULTS
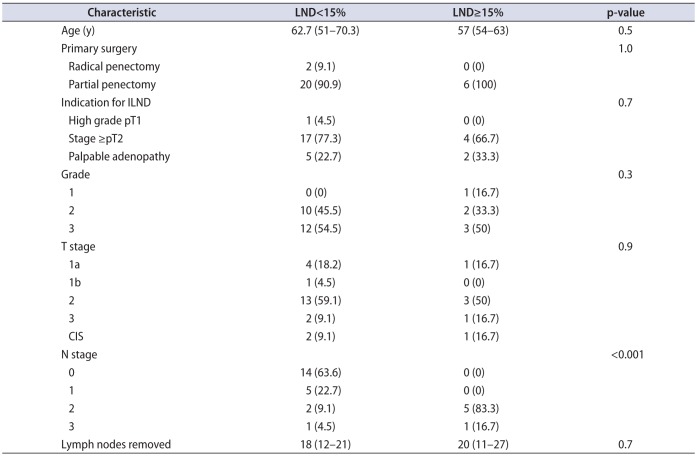
Twenty-eight patients with complete follow-up were identified. Mean follow-up was 34 months (range, 1–174 months). Table 1 lists the clinicopathologic characteristics of the cohort. Indications for ILND were stage >pT2 in 20 patients (71.4%), palpable adenopathy in 7 (25%), and high grade T1 in 1 (3.6%). Of the patients with palpable lymph nodes, none had fixed nodes on physical exam. No patients underwent neoadjuvant chemotherapy or radiation therapy preoperatively. Two patients underwent salvage chemotherapy after recurrence, and 6 patients underwent pelvic lymph node dissection for clinically enlarged pelvic lymph nodes.
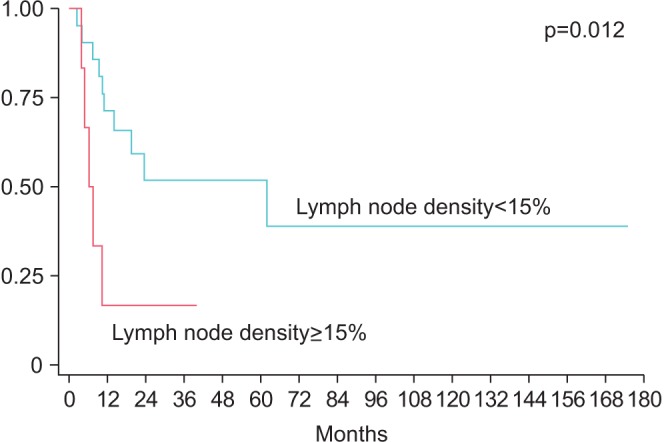
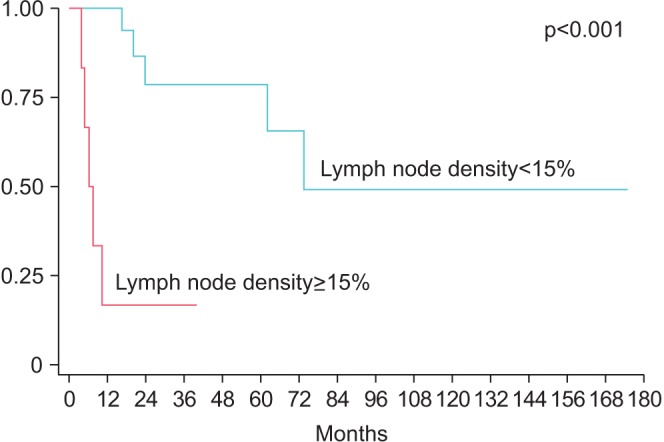
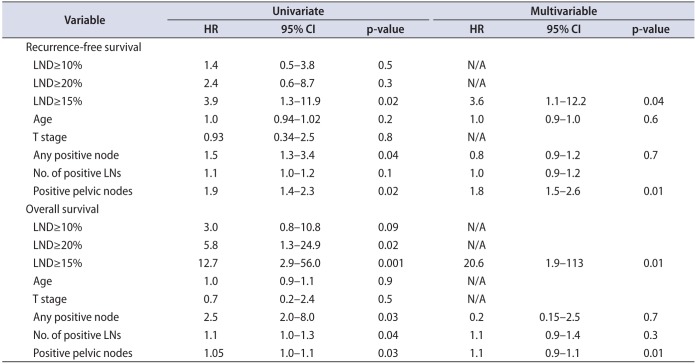
Median node yield after ILND was 17.5 (IQR, 12−22), and positive lymph nodes were found in 14 patients (50%). LND was >10% in 10 patients, >15% in six patients, >20% in 4 patients. LND thresholds of 10% and 20% were not predictive of RFS (p=0.57 and p=0.15, respectively), however RFS was significantly lower for patients with >15% LND (median survival: 62 months vs. 6.3 months, p=0.0120) (Fig. 1). Actuarial 5-year RFS was 51.9% for patients with LND<15% vs. 0% for patients with LND>15%. Similarly, OS was lower in patients with LND>15% (median OS: 73.6 months vs. 6.3 months, p<0.001) (Fig. 2). Actuarial 5-year OS was 78.7% for patients with LND<15% vs. 0% for patients with LND>15%. In a univariate Cox proportional hazard model, LND>15% was predictive of RFS (hazard ratio [HR], 3.9; 95% confidence interval [CI], 1.3–11.9, p=0.019) and OS (HR, 12.7; 95% CI, 2.9–56.0; p=0.001). Absolute number of positive lymph nodes was predictive of OS (HR, 1.14; 95% CI, 1.01–1.30; p=0.037), but not predictive of RFS (HR, 1.1; 95% CI, 0.96–1.23; p=0.18) or OS. Total LNs removed did not correlate with either RFS or OS. Controlling for age, medical comorbidities, number of positive LN, positive pelvic LN, T stage and indication, LND>15% was independently associated with worse RFS (HR, 3.6; 95% CI, 1.1–12.2; p=0.04) and OS (HR, 73.6; 95% CI, 4.8–113; p=0.002) (Table 2). Absolute number of positive lymph nodes was not predictive of OS or RFS in the multivariate model. Harrel c index for RFS was 0.64 for LND compared to 0.54 for total positive LN, indicating a 10% higher concordance for LND and RFS, than total positive LN and RFS. Likewise, the c index for OS was 0.79 for LND compared to 0.61 for for total positive LN, indicating an 18% higher concordance.
DISCUSSION
The presence and extent of disease in the inguinal lymph nodes is the most prognostic factor for survival in penile cancer [123]. In the current study, we validate the observation that LND is a predictor of worse disease. However, initial studies have shown LND cutoffs varied widely in the cutoff used to differentiate worse prognosis [13141516]. Our results identified that a cutoff LND>15% was associated with poorer prognosis. Our data provide further validation of LND's use as a prognostic tool for penile cancer and corroborates a relevant cutoff for clinical use. More significantly, we found that LND outperformed total number of positive lymph nodes both in multivariate Cox proportional hazard model and using Harrel C index for both RFS and OS.
LND's value exists in the combination of both nodal disease burden and extent of LND in a single variable. Nodal burden, represented as number of positive LN, has been shown to be associated with poorer prognosis [71112]. Pandey et al. [2] identified a 75.6%, 8.4%, and 0% 5-year survival with patients who had 1–3, 4–5, and >5 nodes, respectively. However, in this study we did not find an association with total positive nodes removed and RFS or OS. Similar to other solid tumors [17181920], LND has been shown to be a better prognostic tool than LN number as well as the current TNM staging [15] for penile cancer which can account for extent of ILND. The limited studies investigating LND have identified a survival cutoff, which has ranged widely from 6.7%–33% to differentiate favorable versus poor prognosis [13141516]. Our results fall within the wide range of cutoff values and show RFS was significantly worse with LND>15%.
Our results are very similar to Li et al. [13] and Lughezzani et al. [14] who identified LND cutoffs of 16% and 22%, respectively, to delineate poor versus favorable prognosis. Li et al. [13], in a cohort of 71 pN+ patients, showed the 16% LND cutoff separated a 5-year disease-specific survival (DSS) of 81.2% and 24.4% which in multivariate analysis was also independently associated with worse DSS with a HR of 4.31. These outcomes are similar to our 5-year RFS outcomes of 51.9% for patients with LND<15% vs 0% for patients with LND>15%. Similarly, Lughezzani et al. [14] identified on multivariate analysis that patients with LND≥22% had a 4.55-fold worse CSS. These studies matched our HR of 5.5 for RSS in our multivariate analysis when using a LND>15%. Interestingly, a higher LN threshold of 20% was not associated with RFS in our study, but this was likely due to the small number of patients with LND>20%.
Zhu et al. [16], using patients from the Surveillance, Epidemiology and End Results database, calculated a LND cutoff of 33%, however a significant proportion of their patients had insufficient lymph node dissections. While their median lymph nodes removed (16 LN) was nearly identical to ours (17.5 LN), the IQR of 5 to 27.7 LNs highlighted the inadequacy of many lymph node dissections which would both falsely elevate LND calculations as well as skew survival statistics. Svatek et al. [15] similarly affected its LND denominator with the inclusion of LNs received from pelvic lymph node dissections in 33% of patients, which explains the exceedingly high 32 median nodes removed (IQR, 21–38). Furthermore, the authors stratified survival outcomes simply based on its median LND of 6.7%, which limits its clinical applicability.
In our study, as well as the majority of papers, LND cutoff was calculated based on the identification of the LND value of maximal significance. While this method of choosing a cutoff has clinical utility for both clinicians and patients for survival prognostication, it may not be well suited for guiding practical decision-making. A more suitable LND cutoff would be aimed at the identification of a threshold value associated with low risk disease, represented by a very low recurrence rate. Lughezzani et al. [14] attempted to ascertain a more clinically relevant LND cutoff by using a 20% 5-year recurrence probability as a target for low risk disease. However the 5% LND cutoff used did not reach statistical significance, highlighting the size limitation of many penile cancer patient cohorts. Larger, prospective studies are required to calculate a clinically useful LND cutoff prior to its use in treatment algorithms to guide more extensive lymph node dissection, adjuvant therapy, as well as surveillance protocols.
There are some technical challenges to use LND that are worth noting. In patients with bulky adenopathy, nodes can be matted and an accurate node number cannot be determined. Our study population did not include any patients with matted nodes that could skew our calculations. Another potential challenge is the manner in which the tissue is processed. If there is an attempt to isolate lymph nodes from fibroadipose tissue, small positive could be overlooked. Our institutional practice is to completely embed all tissue which we believe allows a more thorough analysis.
Our study was limited by the retrospective nature as well as the small size of our patient cohort and may limit the prognostic significance of our results. Additionally, during the study period, it was the practice at our institution to proceed to ILND in patients with high-risk features or palpable adenopathy, thus the use of neoadjuvant chemotherapy may influence results of LND in other cohorts who use this multimodal approach. Our previous practice patterns were to use salvage chemotherapy at the first sign of new local recurrence or distant metastatic disease, thus more aggressive utilization of adjuvant chemotherapy may also influence the results of this study. Since 2012, we have increased our utilization of adjuvant chemotherapy in men with lymph node positive disease. The evolving management of penile cancer may change the prognostic significance of our LND cutoff, and additional studies are needed to validate this finding in other cohorts.
CONCLUSIONS
In our small, retrospective cohort, we identified a LND> 15% as being associated with worse RFS, providing further evidence of LND's use as a predictive tool for penile cancer. Multi-institutional studies are needed to identify clinically relevant prognostic data for this uncommon disease.
 XML Download
XML Download