

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Prostate cancer (PCa) screening leads to a 21% to 30% reduction in disease-specific mortality [12]. However, screening and early detection also lead to the diagnosis of clinically insignificant disease, which can result in overdiagnosis and overtreatment [34]. In 2012, the US Preventive Services Task Force (USPSTF) discouraged prostate-specific antigen (PSA)-based PCa screening [5].
Currently, the literature on active surveillance (AS) outcomes is largely from Western countries. There is an established disparity in incidence and PCa aggressiveness between Western and Asian nations [6], which brings into question the safety and efficacy of AS in Asia. Klotz et al. [7] reported the 10-year cancer-specific survival for AS to be 97.2%, which is comparable to that for robot-assisted laparoscopic radical prostatectomy (RALP). Long-term results of AS have already been published in the United States and Europe [8].
AS is now mandatory, not optional, for low-grade PCa. However, in African American men, the progression risk is significantly increased with AS. The pathology outcome in African American men who qualify for AS but elect immediate surgery suggests that African American men have a tendency for more aggressive disease [9]. For a similar reason, AS is rarely utilized in Korea, because pathological upgrading and upstaging of patients eligible for AS were reported to be much higher after RALP than the corresponding rates in Western countries [101112]. The rates of misclassification varied from 44.5% to 54.8%.
Thus, currently available AS criteria might not be suitable in Korean patients. We need to use stricter criteria for AS than used in Western countries. Therefore, there are limited data to inform the safety of AS in Korean men. Data are also lacking to assess the risk and determine the safety of AS. We have used AS for low-risk PCa from 2008 and our 5 years of experience was reported in 2014 [13]. This report represents an update and reanalysis of our experience of AS [13]. These data can be used to revise the strategy for follow-up and definitive treatment by AS.
Go to : 
MATERIALS AND METHODS
A cohort study was initiated in January 2008. Patients were enrolled in this study when they met our inclusion criteria for histologically well-defined, newly developed PCa.
1. Patient population
Clinical data were collected retrospectively from 80 patients who were treated with AS as a treatment for PCa (approval number: DSMC 2016-10-032).
2. Criteria for AS
The selection criteria for AS included biopsy Gleason sum ≤6 with a single positive core with ≤30% core involvement, clinical stage≤T1c, PSA≤10 ng/mL, and negative magnetic resonance imaging (MRI) results. The 12-core biopsy scheme was done by using transrectal ultrasonography. Patients should have more than 12 cores taken on biopsy. If the number of initial biopsies was less than 12, a second confirmatory biopsy was done, which tended to detect higher-grade cancer that had been missed on the original biopsy. The criteria were not changed after our initial report.
3. Follow-up
PSA was measured every 6 months; prostate biopsies were performed at 1 and then every 2 to 3 years. The confirmatory biopsy after the first year was intended to identify higher-grade cancer that had been missed on the original biopsy [7]. MRI was further included in a follow-up study after our initial report. MRI was performed prior to repeat biopsy. When the MRI detected a positive lesion, targeted biopsy was done. The PSA test interval was increased because PSA was not useful in the prediction of disease progression in our initial experience. During the follow-up, if the patient's age exceeded 80 years, AS was converted to watchful waiting.
4. Prediction of disease progression
Patients were reclassified after prostate biopsy was performed. Earlier prostate biopsy was performed if PSA doubling time (DT) was less than 3 years or suspicious clinical progression was seen. PSA DT was not useful in the prediction of disease progression in our initial experience. Nevertheless, the number of patients was insufficient to evaluate the association between PSA DT and disease progression, so PSA DT was measured after the initial report. PSA DT was calculated by use of the following formula: where A & B are the initial (A) and final (B) PSA measurements and dT is the time difference between the calendar dates of the 2 PSA measurements [14].
5. Criteria for intervention
Definitive intervention was offered to those patients with Gleason score progression (an increase to 7 or greater) or an increase in the number of positive biopsy cores (2 or more than 1 lobe).
6. Statistical methods
Chi-square was used to analyze prediction of disease progression. The Kaplan-Meier method was used to analyze the progression-free survival rates for prostate volume after division into tertile values. Statistical analysis was performed by using IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA). A p-value of <0.05 was taken to be significant.
Go to :
RESULTS
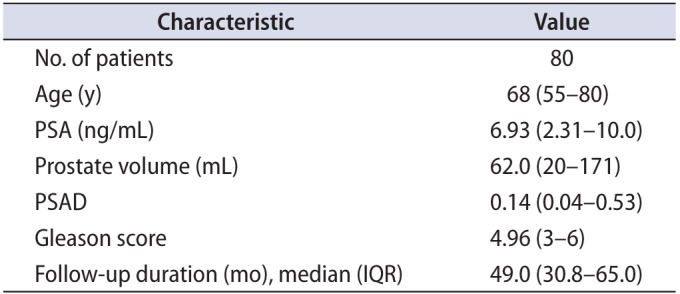
A total of 80 patients were enrolled and treated with AS. The patients' mean age was 68 years (range, 55–80 years), their mean PSA was 6.93 ng/mL (range, 2.31–10.0 ng/mL), their mean prostate volume was 62.0 mL (range, 20–171 mL), their mean Gleason sum was 4.96 (range, 3–6), and their mean PSA density was 0.14 ng/mL (range, 0.04–0.53 ng/mL). Median follow-up duration was 49.0 months (interquartile range, 30.8–65.0 months) (Table 1).
In the first year of follow-up, 50 patients (62.5%) underwent repeat biopsy (43 patients, single core Gleason 6 without progression or negative for cancer; 7 patients, progression). Three patients were lost to follow-up. A total of 15 patients wanted to change the treatment modality before the repeat biopsy. Twelve patients awaited the scheduled first-year follow-up biopsy (some of them were delayed). Of the patients who experienced progression, 5 patients underwent radical prostatectomy, whereas 2 patients requested a transfer to another hospital of their choice.
In the third year of follow-up, repeat biopsies were performed in 21 patients (12 patients, stable; 9 patients, progressed). In the fifth year of follow-up, repeat biopsies were performed in 4 patients (3 patients, stable; 1 patient, progression, treated with radical prostatectomy).
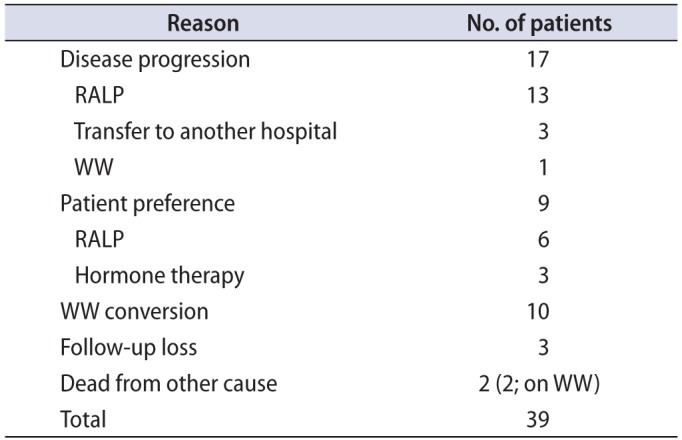
During the entire period, 39 patients (48.8%) discontinued AS for various reasons (17, disease progression [13 RALP, 3 transfer to another hospital, 1 watchful waiting]; 9, patient preference [6 RALP, 3 hormone therapy]; 10, watchful waiting due to old age; 3, follow-up loss; 2, death from other cause). Therefore, 41 patients (51.3%) remained on AS (Fig. 1, Table 2). In the patients who experienced progression, 2 had a Gleason score of 6 with 2 or 3 core involvements, 13 had a Gleason score of 7 with 1 to 7 core involvements, and 2 had a Gleason score of 8 with 2 or 3 core involvements.
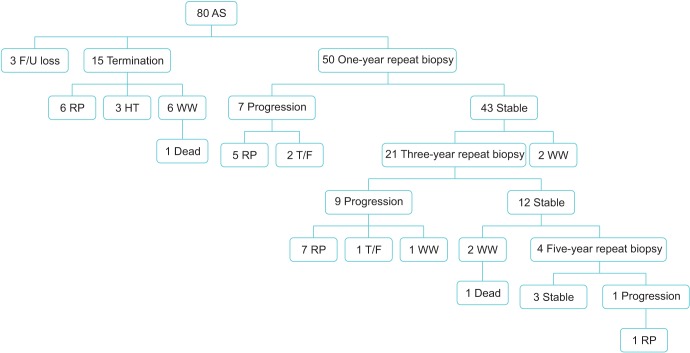 | Fig. 1Flow chart of active surveillance. AS, active surveillance; F/U, follow-up; RP, radical prostatectomy; HT, hormone therapy; T/F, transfer; WW, watchful waiting.
|
The probability of progression was 14.0% (7 of 50 patients) and 42.9% (9 of 21 patients) at 1 and 3 years, respectively. Overall survival was 97.5% (78 of 80 patients). PCa-specific survival was 100%.
RALP was performed in 19 patients. Two patients had extracapsular extended disease (pathologic T3a, Gleason score 3+4 and 4+3). However, there was no recurrence after definitive treatment.
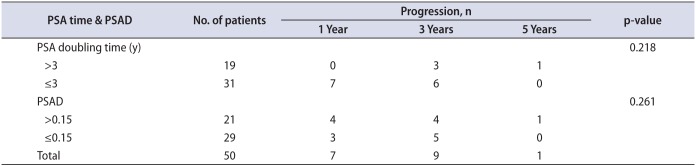
A total of 19 patients underwent prostate biopsy earlier owing to a PSA DT of less than 3 years. However, only 4 of them (21.1%) had cancer progression. A total of 17 patients with disease progression had a mean PSA DT of 9.95 years (Table 3). Progression occurred in 5 of 7 patients (71.4%) with a prostate volume less than 30 mL, 7 of 40 patients (17.5%) with a prostate volume of 30 to 50 mL, and 5 of 33 patients (15.2%) with a prostate volume of 50 mL or larger (Fig. 2). The progression rate was significantly lower in the patients with a larger prostate (p=0.002).
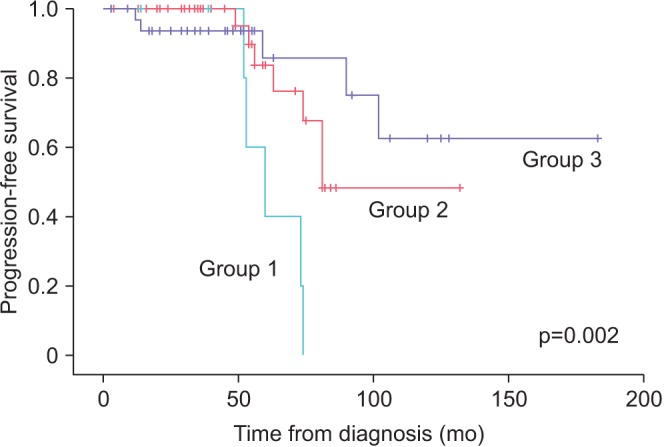 | Fig. 2Progression-free survival for prostate volume. Group 1, prostate volume<30 mL; group 2, prostate volume 30 to 50 mL; group 3, prostate volume≥50 mL.
|
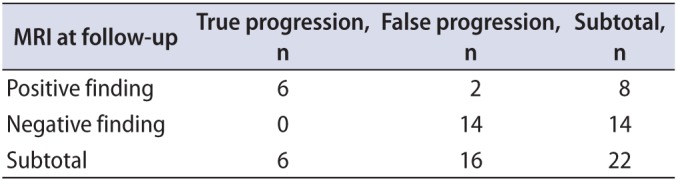
During the follow-up, 22 patients had MRI. There were 8 detectable positive lesions at follow-up MRI. Of them, 6 patients (75.0%) had actual progressed disease (Table 4). Diagnostic properties of MRI to predict progression were sensitivity of 100%, specificity of 87.5%, positive predictive value of 75.0%, and negative predictive value of 100% (Table 5).

Go to :
DISCUSSION
The USPSTF recommendation against PSA screenings was based on concern about overdiagnosis and overtreatment [5]. This message was reinforced by the results of the PIVOT study [15]. Klotz et al. [7] reported the 10-year cancer-specific survival for AS to be 97.2%, which is comparable to that for RALP. AS is mandatory, not optional, for low-grade PCa. AS is an effective method for reducing overtreatment because PCa with a Gleason score of 6 is rarely lethal.
We used the following inclusion criteria for AS in Korea for very-low-risk PCa: biopsy Gleason sum ≤6 with a single positive core, clinical stage≤T1c, PSA≤10 ng/mL, and negative MRI results [16]. Our inclusion criteria were the strictest criteria for AS. AS is rarely used in Korea, because pathological upgrading and upstaging of patients eligible for AS were reported after RALP in comparison with Western countries [10111217]. The rate of upgrading ranged from 41.6% to 50.6%. Extracapsular extension was reported in 4.1% to 8.5%. The rate of upstaging varied from 4.5% to 9.3% and the rates of misclassification varied from 44.5% to 54.8%. Therefore, we did distinguish between low-risk disease and very-low-risk disease. We also used strict definitions of disease progression and intervention criteria.
In our study, the probability of progression was 14.0% (7 of 50 patients) and 42.9% (9 of 21 patients) at 1 and 3 years, respectively, despite the strict inclusion criteria. Nevertheless, overall survival was 97.5% (78 of 80 patients). PCa-specific survival was 100%. Therefore, AS can be used in Korea.
It is difficult to determine the individual risk of disease progression in someone with PCa with Gleason 6. In several recent reports, PSA kinetics has been used to predict disease progression [7]. Klotz et al. [7] also focused on PSA kinetics to determine a definite intervention. However, in our initial experience, PSA was not associated with cancer progression. In the 8-year analysis, PSA DT also could not predict disease progression. After diagnosis, PSA tended to decrease or stabilize in most of the patients with PCa. We think that lifestyle changes made this possible.
In our study, PSA density was not associated with progression. After stratification, prostate volume was related to progression. Progression occurred more often in cases of PCa with a small prostate. The progression rate was significantly lower in patients with a larger prostate (p=0.002). Several studies have reported that higher PSA density at baseline predicts a greater risk of progression [81819]. Tosoian et al. [20] reported in a comparative analysis of men electing AS and immediate surgery that PSA density per 0.1-unit increase was identified as a significant predictor of adverse pathology. Jin et al. [21] also reported PSA density as a strong predictor of Gleason score upgrading after radical prostatectomy in patients eligible for AS. In our study, small prostate volume tended to be associated with cancer progression. However, one limitation of our study was the use of unusual statistics because of the small numbers.
We used MRI at follow-up to determine upgrading and upstaging of PCa. Recently, the usefulness of MRI has been consistently reported [2223]. MRI with various imaging techniques has improved tumor detection. If the tumor has progressed, MRI can be used to detect the lesion. At the beginning of our study, all patients had negative findings for MRI. A total of 22 patients underwent MRI at the yearly follow-up. There were 8 detectable positive lesions on MRI. Of them, 6 patients (75.0%) had actual progressed disease. Henderson et al. [24] focused on MRI in AS and concluded that MRI is a useful marker when selecting patients for AS and may help in predicting whether patients should receive close monitoring or whether immediate treatment should be given. We think that MRI is very useful for selecting patients for AS and for detecting cancer upgrading [25]. Especially, lesions in the apex or anterior of the prostate are difficult to find. In these cases, MRI is useful for identifying occult anterior lesion cancers [26]. However, the purpose of the follow-up MRI in our study was not to detect upgrading or upstaging but to make a decision about early biopsy or to make target biopsy easier. Nevertheless, we believe that every patient undergoing AS should have a repeat biopsy to detect disease progression periodically. PSA kinetics and MRI can miss disease progression. Quon et al. [27] reported the risk of false-positive and false-negative diagnosis of PCa with multiparametric prostate MRI in AS. Lee et al. [28] reported that nonvisible tumors on multiparametric MRI do not predict low-risk PCa. In order to carry out AS safely, a new biomarker or a new tool for detecting disease progression is needed.
AS can minimize overtreatment of indolent PCa and avoid or postpone the side effects of definite therapy. Thus, AS can give quality of life to men with low-risk PCa. Klotz et al. [7] reported the 10-year cancer-specific survival for AS to be 97.2%. In our study, overall survival was 97.5% (78 of 80 patients). Prostate-cancer-specific survival was 100%. Thus, AS is also a feasible treatment option for low-risk PCa patients in Korea.
However, our study had several limitations. First, many patients are reluctant to undergo repeat biopsy and thus postpone follow-up or transfer to another hospital. Second, considering the long life-span of PCa, the total follow-up period of this study was too short to ensure the safety of AS. Third, because of the small numbers, we used unusual statistics. Therefore, further study will be needed.
Go to :
CONCLUSIONS
Early outcomes of AS showed it to be safe and feasible in carefully selected men with very-low-risk PCa in Korea. There was no incurable progression and PCa-specific survival was 100%. As in our first report, PSA DT was not helpful in predicting PCa progression. However, we did know that a small prostate volume is associated with a tendency for cancer progression. MRI showed benefit for the detection of progression. MRI may reduce the rate of serial biopsy and improve the early identification of occult high-grade disease. Nevertheless, regular biopsies should be performed. Further study is needed to reduce the number of biopsies. Also, longer follow-up is needed to assess the effectiveness of AS.
Go to :
 XML Download
XML Download