

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Radical prostatectomy has historically been the preferred treatment option for patients with localized prostate cancer. However, surgical innovations to reduce blood loss and hasten the recovery rate have led to the introduction of laparoscopic radical prostatectomy (LRP) followed by robot-assisted radical prostatectomy (RARP) as alternatives to open surgery [12]. RARP was introduced to decrease the difficulty in performing complex laparoscopic procedures such as urethral anastomosis. The robotic platform provided several advantages over LRP, such as seven degrees of freedom, tremor filtration, a three-dimensional magnified view, and preferred ergonomics [3]. Therefore, robot-assisted surgery has become popular in Korea, the United States, and Europe [14]. However, this trend has occurred despite a lack of high-quality evidence supporting improvement in outcomes.
Randomized controlled trials comparing the safety and effectiveness of RARP and LRP are limited. Therefore, high-level evidence is a requisite for clinicians needing recent evidence on the treatment of prostate cancer. The primary objective of this study was to determine whether RARP is more effective than LRP in the treatment of prostate cancer in terms of functional, oncological, and perioperative outcomes.
MATERIALS AND METHODS
1. Inclusion criteria
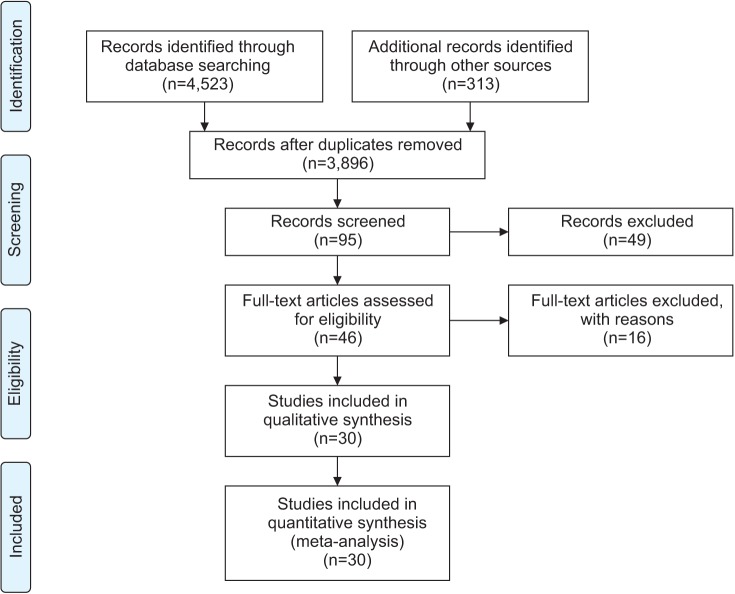
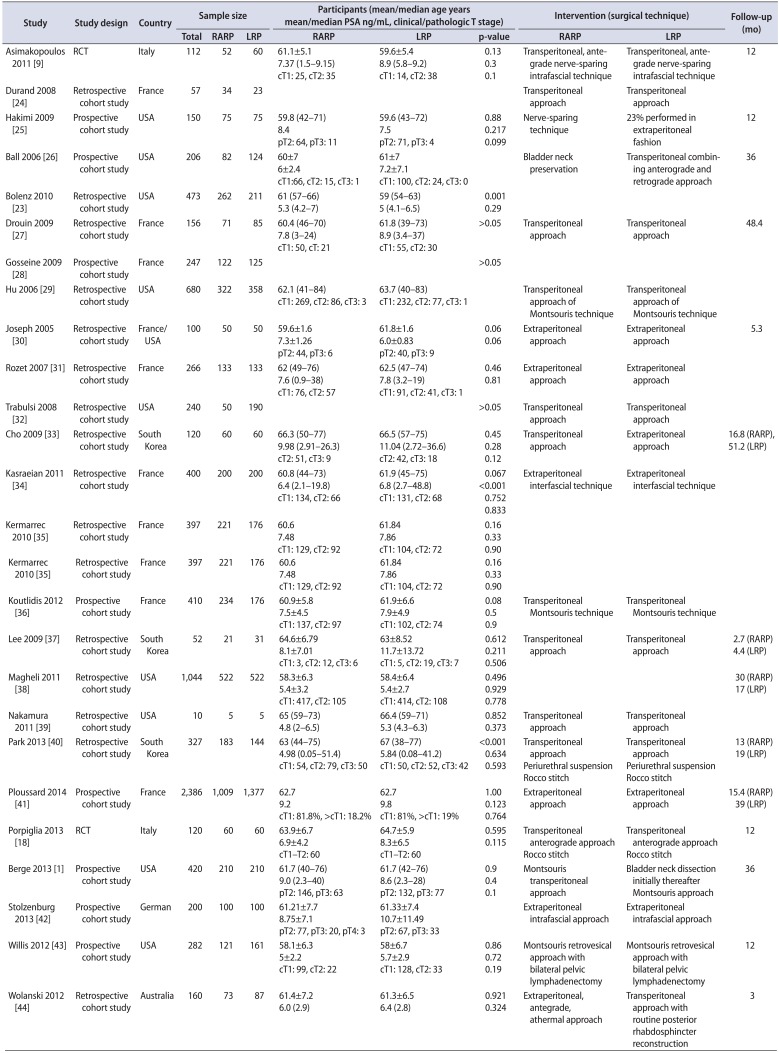
Eligible studies included randomized controlled trials and prospective and retrospective cohort studies comparing RARP and LRP. A study was excluded if it did not report any outcomes of interest or functional and oncological outcomes.
2. Search strategy
We searched electronic databases for reviews published through July 2014, including Ovid MEDLINE (Ovid, New York, NY, USA), Ovid EMBASE (Ovid), the Cochrane Library (London, United Kingdom), KoreaMed (KAMJE, Seoul, Korea), Kmbase (MedRIC, Chungbuk, Korea), KISS (Korean Studies Information Co, Paju, Korea), RISS (KERIS, Daegu, Korea), and KisTi (KISTI, Daejeon, Korea). Patient-related search terms (prostatic neoplasm, prostatic cancer, prostatic carcinoma, prostatic tumor), and intervention-related search terms (robotics, computer-assisted surgery, telerobot, remote operation, remote surgery, da Vinci) were combined.
3. Data synthesis and analysis
Two independent reviewers selected the studies, extracted data, and performed quality assessments. The authors assessed the relevance and quality of the selected systematic reviews related to the research question through the revised assessment of multiple systematic reviews (R-Amstar). For the prospective randomized controlled clinical studies, the Cochrane Collaboration's tool for assessing risk of bias was used to perform the quality evaluations. For the nonrandomized studies on the final selected literature, a revised risk of bias was used to perform the quality evaluations. Functional and oncologic outcomes, as well as postoperative complications and perioperative results (operation duration, length of stay), were calculated and compared between the groups.
4. Statistical analysis
Meta-analysis was conducted by using RevMan 5.2 (Cochrane Community, London, United Kingdom) and Comprehensive Meta-Analysis 2.0 (CMA; Biostat, Englewood, NJ, USA). The Cochrane Q and I2 statistics were used to assess statistical heterogeneity. The results were expressed as weighted means and standardized mean differences for continuous outcomes and as relative risk (RR) and 95% confidence intervals (CIs) for dichotomous variables. For dichotomous variables, the random effect model of Mantel-Haenszel was used, and for continuous data, the random effect model of the inverse-variance method was used. Publication bias was tested by using a funnel plot and Egger's test. The statistical analyses were reviewed by a statistician with previous meta-analysis experience.
6. Quality assessment
For the RCTs, there was a low risk of bias in sequence generation, blinding, selective report, and other biases. However, the allocation of concealment was uncertain, and incomplete outcome data were at a high risk of bias. In the cohort studies, sequence generation and allocation of concealment, which are important factors in the quality assessment of therapeutic publications, were at a high risk of bias.
RESULTS
1. Postoperative complications
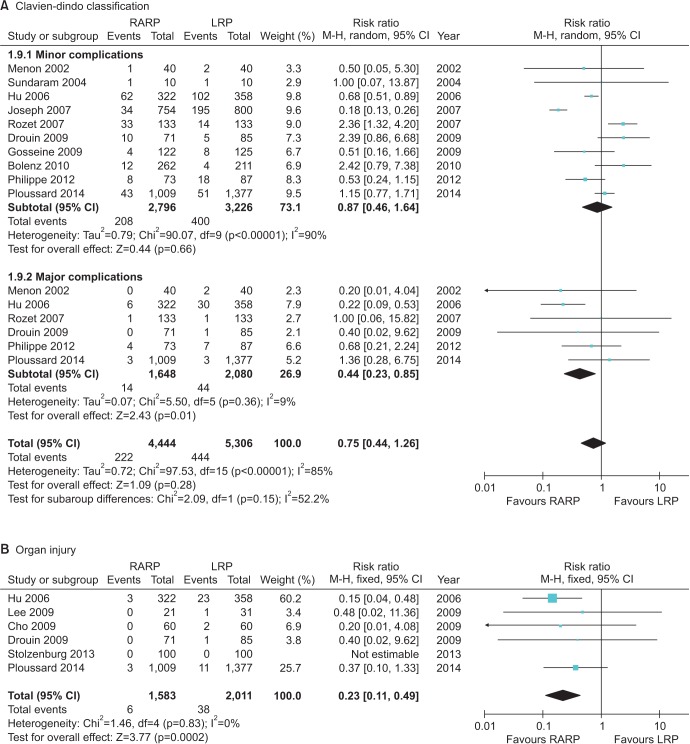
The risk of complications, such as bladder neck contracture (RR, 0.40; 95% CI, 0.17–0.92; p=0.03), organ injury (RR, 0.23; 95% CI, 0.11–0.49; p=0.0002), and other major complications (Clavien-Dindo III–V) according to the Clavien-Dindo classification (RR, 0.44; 95% CI, 0.23–0.85; p=0.01), was lower for RARP than for LRP. Anastomosis site leakage (RR, 0.67; 95% CI, 0.42–1.08; p=0.10) and the rates of infection (RR, 1.21; 95% CI, 0.84–1.76; p=0.31), ileus (RR, 0.73; 95% CI, 0.38–1.40; p=0.34), and pulmonary embolism (RR, 1.20; 95% CI, 0.22–6.51; p=0.83) were not significantly different between the groups (Fig. 2). No significant difference in the conversion rate (RR, 0.70; 95% CI, 0.25–1.95; p=0.50) was observed. RARP carried a lower risk of transfusion than LRP (RR, 0.70; 95% CI, 0.54–0.91; I2=44%; p=0.007).
2. Perioperative data
The operation time for RARP was shorter than that for LRP (RR, −18.74; 95% CI, −32.15 to −5.33; p=0.006), but the statistical heterogeneity was high (χ2=527.29, df=22, p<0.00001, I2=96%). The hospital stay following RARP was 1.53 days shorter than that following LRP. The results of the subgroup analysis according to region showed a mean difference of −1.13 (95% CI, 2.93–0.67; p=0.22) in the Asia Pacific region, −0.56 (95% CI, 1.14–0.02; p=0.06) in the United States, and 0.32 (95% CI, 0.88–0.25; p=0.28) in Europe. However, the overall statistical heterogeneity was high (I2=94%).
3. Functional outcomes
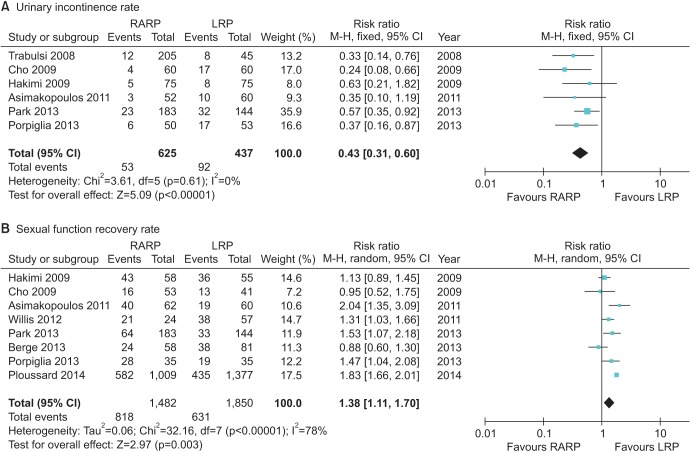
The functional outcomes were improved in a comparison between RARP and LRP (Fig. 3). The urinary incontinence rate at 12 months was lower for RARP than for LRP (RR, 0.43; 95% CI, 0.31–0.60; p<0.000001), and statistical heterogeneity was low (I2=0%). The potency recovery rate was higher for RARP than for LRP at postoperative 12 months (RR, 1.38; 95% CI, 1.11–1.70; I2=78%; p=0.003). Potency recovery was defined as an International Index of Erectile Function 5 (IIEF-5)>17.
4. Oncologic outcomes
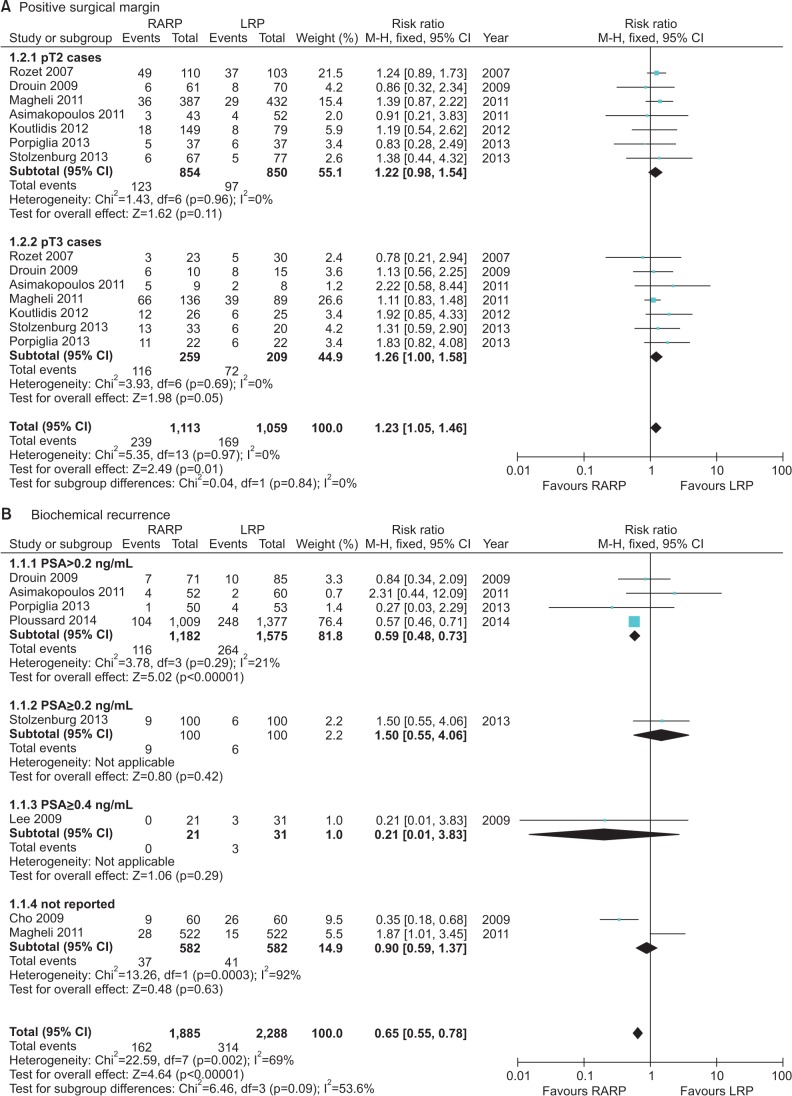
The overall positive surgical margin (PSM) results were investigated in 7 studies. When analyzing PSM rates in the pT2 group, the RARP and LRP series had PSM rates of 14.2% (123 of 864 cases) and 11.3% (97 of 860 cases) with an RR of 1.22 (95% CI, 0.98–1.54; p=0.11). In the pT3 group, the PSM rates for RARP and LRP were 43.1% (116 of 269 cases) and 34.4% (72 of 209 cases) with an RR of 1.26 (95% CI, 1.00–1.58; p=0.05) (Fig. 4).
The biochemical recurrence (BCR) rate was significantly lower for RARP than for LRP (RR, 0.59; 95% CI, 0.48–0.73; I2=0%; p<0.00001) (Fig. 4). Five studies used prostate-specific antigen (PSA)≥0.2 ng/mL to indicate BCR, 1 study used PSA≥0.4 ng/mL, and 2 studies did not define the cutoff used. The follow-up period ranged from 3 months to 60 months. The overall BCR rates for RARP and LRP were 8.6% (162 of 1,885 cases) and 13.7% (314 of 2,288 cases).
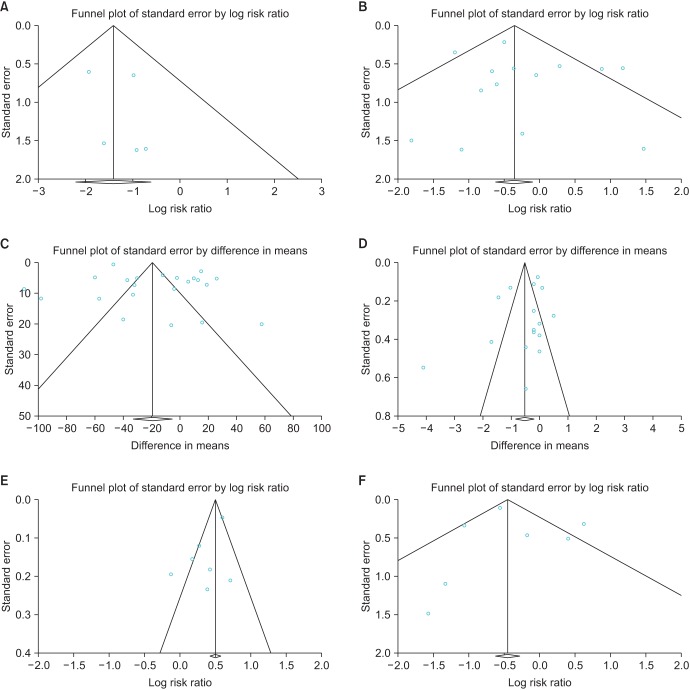
5. Publication bias
A funnel plot analysis for organ injury, blood transfusion rate, length of stay, potency, and overall BCR revealed a symmetrical funnel plot, indicating no publication bias (Fig. 5) (p=0.53, p=0.47, p=0.26, p=0.10, and p=0.70, respectively, Egger test). However, operative time revealed asymmetry on the funnel plot (p=0.01, Egger test).
DISCUSSION
Our study revealed three important findings: (1) the risk of complications after RARP was significantly lower than after LRP; (2) in comparison with LRP, the risk of urinary incontinence at 12 months was significantly lower and the potency rate was higher with RARP; (3) the BCR rate was significantly lower after RARP than after LRP.
The major findings of this meta-analysis showed significant differences in complications such as organ injury and other major complications according to the Clavien-Dindo (III–V) classification. The major complication rate was significantly lower for RARP than for LRP. Although both laparoscopic and robotic surgeries are regarded as minimally invasive techniques, the main advantages of RARP, such as seven degrees of freedom in robotic arm movement and magnified 3D vision of the robotic platform, result in decreased postoperative complications.
Incontinence is another complication of prostatectomy that greatly affects quality of life [5]. The urinary incontinence rate is influenced by the definition of incontinence. Thus, as reported previously, any systematic review is difficult to accomplish owing to the varying definitions used for urinary incontinence, such as involuntary urine loss [6], needing zero or 1 pad [7], and also those in the International Consultation on Incontinence Questionnaire-Short Form survey [8].
The urinary incontinence rate after 12 months was significantly lower with RARP than with LRP in this meta-analysis and in other randomized controlled trials, in which the rates for RARP and LRP were 6% and 17%, respectively, but without statistical significance owing to the limited study population [9]. Many modifications have been suggested in the field of robotics to improve the continence rate. Patel et al. [10] reported a peri-urethral suspension suture technique to improve the rate (92.8% vs. 83%; p=0.013 over 3 months). A modified posterior reconstruction that increased the continence rate by 4 weeks was reported by Coelho et al. [11]. In 2011, Asimakopoulos et al. [9] suggested a pubovesical-complex-sparing technique, in which a ventral plane was developed between the detrusor apron and the prostate. Owing to the technical feasibility of robotic assistance, reconstruction procedures have additionally improved the continence rate.
The potency recovery rate is another major concern for patients undergoing prostatectomy. The most common reason for failure to reach pentafecta is erectile dysfunction (35%) [12]. Our findings differed from those previously reported by NETSCC (2012), which showed no difference in the potency rate between RARP and LRP at 12 months postoperatively. In our meta-analysis, the potency rate of RARP at 12 months was significantly higher than that for LRP. Different potency recovery rates could be due to several factors, including different definitions of erectile dysfunction, various characteristics of the surgery, and differences in postsurgical rehabilitation [13]. Potency recovery was measured by using several methods, including the IIEF-5 and the Sexual Health Inventory for Men score. Various techniques for preserving potency have been developed on the robotic platform, including cavernous nerve preservation. Several nerve-sparing techniques were developed in previous studies. For example, Ahlering et al. [4] evaluated the adverse effects of electrocautery on dissection of the prostate and the superiority of cautery-free nerve-sparing techniques on the recovery of potency. Menon et al. [14] evaluated the “Veil of Aphrodite” technique in which the inter-fascial plane was extended towards the apex and laterally towards the prostatic pedicle. At 6 to 18 months postoperatively, 94% of men who attempted sexual intercourse after undergoing this technique reported success, with a median SHIM score of 18 out of 25. Following recent discoveries of the periprostatic fascial anatomy, extrafascial, interfascial, and intrafascial approaches have been developed. Comparing inter-fascial and extrafascial approaches, Shikanov et al. [15] reported a significantly improved potency rate (p=0.03) using the interfascial approach.
Three-dimensional magnified visualization of the robotic platform has enabled meticulous dissection of the periprostatic fascia layer and the neurovascular bundle. Further insights into the multilayered structure of the periprostatic fascia and the course of the cavernous nerves have supported the development of intra- or interfascial surgical planes, which have enabled improved functional outcomes in urinary incontinence and potency. A PSA level>0.2 ng/mL was selected as the important criterion, based on recommendations of clinical practice guidelines [16]. In an oncological RARP study, Menon et al. [17] reported biochemical-free survival rates of 95.1%, 90.6%, 86.6%, and 81.0% after 1, 3, 5, and 7 years, respectively. Few studies have reported BCR rates after RARP and LRP. Recently, Porpiglia et al. [18] reported BCR-free survival rates of 98% for a RARP group and 92.5% for an LRP group (p=0.190).
The oncologic outcome in the current study was noteworthy because of the statistically signif icant differences in BCR rates between the two groups. Ficarra et al. [13] demonstrated that BCR was significantly influenced by surgical experience, clinical tumor size, and anatomic tumor characteristics. Kim et al. [19] analyzed the preoperative predictors of BCR using multivariable analysis, which suggested that PSA, pathologic stage, pathologic Gleason score, and PSM were independently associated with BCR. In a Japanese study, the predictive factors of BCR following RARP were serum PSA levels, the percentage of positive cores, and the Gleason score. PSA density was also a strong predictor of advanced pathological features and BCR [20]. In our systematic review, the oncologic results for BCR showed a statistically significantly improved BCR in the RARP group relative to the LRP group, although the propensity score matching was similar between the groups. The PSM patients in the intermediate- and high-risk disease groups had higher rates of BCR than did those who were marginal or negative. However, the PSM in the low-risk disease group was not associated with disease progression [21]. After adjustment for differences in clinical and pathological features, the presence of a base margin was significantly associated with a shorter time to recurrence for intermediate- and high-risk disease. The apex margin also was associated with the time to recurrence, but not statistically so for intermediate-risk disease. Thus, the similar PSM rate did not indicate a similar BCR rate. The length of the PSM was also independently predictive of BCR. Patients with a PSM <1 mm appeared to have similar outcomes compared with those with negative surgical margins [22]. Patients with a PSM <1 mm did not differ from those with a negative margin, and as the length of the positive margin increased so did the risk of BCR. Interestingly, the risk of BCR did not differ between patients with a negative surgical margin and those with a PSM <1 mm.
The current study had several limitations. First, because this is a relatively new procedure, data were lacking on long-term oncologic results following RARP, such as the cancer-specific survival rate. Second, significant heterogeneity was evident in terms of surgical experience and definition of functional outcomes. Third, some of recently published articles had far larger cohorts, which strongly influenced the meta-analysis. Fourth, there was an era bias in several centers in that RARP was performed after LRP.
CONCLUSIONS
In conclusion, RARP showed favorable results compared with LRP. However, few long-term, high-quality studies are available comparing RARP and LRP. Although further studies are needed, our results revealed that RARP had an improved BCR rate, potency rate, and continence rate with fewer complications than LRP. Further high-quality studies that minimize confounding and selection biases with long-term follow-up are needed to further clarify the clinical efficacy and safety of RARP.
 XML Download
XML Download