

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The prevalence of overactive bladder (OAB) is not less than 46.9% in men, and no less than 61.0% in women older than 65 years [1]. Intrusive and annoying OAB symptoms reduce the health-related quality of life, suppress social activity, often lead to depression and psychological discomfort [23]. OAB treatment is associated with significant expenses for the purchase of medicines [4]. Antimuscarinic (AM) drugs are the main way to manage OAB symptoms in the older [56].
Studying AM drugs' efficacy and safety in previous studies, we have seen poor adherence to treatment with this drug class in older patients [78], which is consistent with the other authors' data [910]. Pharmacological properties of AMs providing clinical effect are considered to be the main factors determining patient's adherence [1112]. However, some researchers believe that adherence to AMs is poor regardless of a particular drug, and their pharmacological properties are not the only patients' adherence control [13]. The patients' adherence increases in older age with a good awareness of their disease [1415]. Several researchers present data on significant influence on adherence to AM treatment of factors such as the drug cost [16], the income level, expense interest on AMs and other drugs, as well as disability, depression and psycho-emotional problems caused by a decrease in the social adaptation level [17181920]. Some researchers indicate the lack of a systematic approach studying the influence on the adherence of various factors, as well as the complexity of its objective evaluation [21], the need to study the “rational nonadherence to regime” and a discrepancy between reasons for the refusal of treatment indicated by patients and actual motivation [22]. A more faithful representation of real reasons for the refusal to continue therapy could facilitate for practicing urologists prediction of prescription compliance and the justification of a choice, as well as, possibly, identify the need for consultation by psychologists, psychotherapists, social workers and other specialists.
Given these circumstances, we have formulated an objective – to compare subjective reasons for the refusal of AM drug treatment and objective health status markers related to OAB, patients' socio-economic status.
MATERIALS AND METHODS
1. Study design and patients
The prospective study was conducted from September 1, 2013 until March 18, 2015 housed by the city polyclinic No. 3 (Vladivostok city) and the Far Eastern Federal University. The 1,736 individuals aged over 60 years participated in the experiment (59.7% of women, 40.3% of men). Calculating the sample size a 95% confidence level (a±5% interval) was determined. In view of the homogeneity and the volume of the population for selection of patients systematic random sampling was used, ordered on the basis of AM drugs taking. The calculation was carried out taking into account the likely amount of loss of contact with patients from the experience of previous studies having similar design. In order to ensure meaningful comparison between the groups at the finish of the study the target number of patients was 1,736 people. The number of lost contacts has not exceeded the estimated rate.
The group included individuals who sought medical advice from an urologist concerning OAB (CM N32.81) [23] in odd-numbered days of the month, and who got AM drugs prescribed (oxybutynin, tolterodine, trospium, solifenacin, darifenacin) as a permanent maintenance therapy [56]. Exclusion criteria were simultaneous administration by patients of other anticholinergic drugs, reception of AM drug within 3 months before the study, a history of acute urinary retention related to the AM drug administration, the presence of terminal cancer, a chronic infection of lower urinary tact, changes in the QT interval.
In the course of the experiment, we complied with principles of the Declaration of Helsinki. All participants of the experiment have given written informed consent. The study protocol was approved by the ethics committee for Applied Scientific Research FEFU (2013/2/00134FEFURU).
2. Measures adherence
The adherence evaluation was carried out using the model of waiting for a 30-day break in the AM drugs administration [1922]. In accordance with the adherence level all patients were divided into 2 cohorts – adherent (patients complied with prescriptions ≥80% of the follow-up period) and poorly adherent (<80%) [19]. We have identified parameters significantly different in different cohorts as objective social, economic, psychological status markers [192122] and markers of the detrusor functional activity [24]. Then, we compared the percentage of individuals having at least one of these parameters not consistent with average sample values with the percentage of individuals indicated a specific reason for the refusal of further therapy.
3. Data collection
An objective evaluation of the functional state of the lower urinary tract and the efficacy of the treatment was carried out using monthly overactive bladder questionnaire short form and uroflowmetry [2526], daily filling by patients of voiding diaries, supplemented by columns containing information on the AM drugs administration and side effects [27] as well as data on the AM prescribing from a patient's medical record. The presence of scored episodes of urgent urination and urinary incontinence, severity of symptoms, estimated by the number of episodes of urinary incontinence per week, the average urine flow rate, the average bladder volume were markers of the functional state of the lower urinary tract. The OAB symptoms were evaluated in the presence of heavy urinary incontinence episodes more than 3 times a day on average [28]. Control of economic status was performed according to income documents from the Tax Inspectorate received after patients' written informed consent to provide information, as well as checks, evidencing payments for medicines and certificates from the Social Security Service. Calculation of the income level and expenses is presented adjusted for inflation from the conversion of the national currency according to the United States dollar price as of August 2013 [19]. Annual income, average monthly income, annual additional income, annual medical cost, expenses on AM-drug (%), annual expenses on other drugs, short-term and long-term disability days were markers of the economic status. Social functioning, physical functioning, role-emotional, role-physical, mental health (Medical Outcomes Survey 36-item Shor-Form Health Survey, monthly) were markers of self-assessment of the social and psychological status [29].
Any reason for the refusal to continue therapy, associated with severe manifestation of OAB symptoms, AM drugs' efficacy, the presence of side effects, the dissatisfaction with administration mode were identified as medical. Sometimes, the complete disappearance of OAB symptoms, i.e., the “cure” as realized by a patient was identified as a reason for refusal, which also was verified as a medical reason for the refusal [9,11,13]. By economic reasons are meant references to the low income level, the need for substantial expenses on drugs and medical services, etc. [1920]. If indicated reasons for the refusal included AM drug administration anxiety, the aversion to AM drugs, prior confidence in its inefficacy, the lack of social support from family members, friends, the limitation of social contacts related to the need to use pads, obsessive fear of unpleasant odor spreading, etc., we verified these reasons as a sociopsychological [20]. When analyzing data obtained, we have also studied reasons for refusal in specific individuals with objective changes in certain parameters.
4. Statistical analysis
The statistical analyses were performed using SAS ver. 8.0.2 (SAS Institute Inc., Cary, NC, USA). To evaluate the feature (adherence) survival time we used the Weibull distribution with the right censoring type 1 and the result adjustment using Hollaender-Proschan test, as well as the building and analysis of signs' regression models.
RESULTS
Fifty-two point six percent (52.6%) of patients preserved adherence to treatment during the first 6 months, 30.1% – during the follow-up period. The average time of reaching a 30-day break in the AM drugs administration was 174 days.
Table 1 provides main demographic characteristics of cohorts with the high and moderate adherence level. Table 2 provides regression-adjusted economic characteristics and their comparison between the cohorts with <80% and ≥80% adherence. Average annual income and annual medical cost were statistically significantly higher (p≤0.05, p≤0.05), and average expenses on AM drug were lower (p≤0.05) in a cohort of adherent patients.
Table 3 provides regression-adjusted medical characteristics, as well as markers of health effect on the quality of life in older patients with different levels of adherence to treatment at the moment of discontinuing the AM drugs administration. Urge, urinary incontinence, average volume rate of urination (Qaver), bladder volume values, as well as the percentage of patients with side effects in cohorts with different adherence levels were significantly different (p≤0.05, p≤0.05, p≤0.01, p≤0.05, p≤0.01, respectively). Also, when evaluating social functioning, role-emotional and rolephysical scores were significantly different (p≤0.05, p≤0.05, p≤0.05). The most common psychological reasons associated with poor adherence we had to deal with during our study were the absence of significant social support from close relatives, distrust of AM (especially among individuals using these drugs for the first time), fear of possible side effects (usually it was extrapolation of negative experience in treatment with drugs of other groups), preference of nondrug therapy, disbelief in the possibility of cure. In some cases, there has been prepossession against the physician prescribing treatment. Also, in several cases, refusals were motivated by the presence of a good therapeutic effect, and belief that further treatment is meaningless or harmful.
Then, we assumed that parameters and characteristics varying in individuals with different adherence levels may be important for the comparison of their objective status with subjective reasons for the refusal of treatment [19].
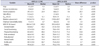
Table 4 provides objective characteristics of health, economic and socio-psychological status of patients indicated different reasons for the refusal of treatment. Among patients reported medical reasons for the refusal of treatment (subgroup 1) Urinary incontinence level is higher than in the group of patients reported economic reasons (p≤0.05), and is statistically homogeneous with respect to subgroup 3 and average values of the whole sample. In this subgroup, the percentage of side effects is significantly higher compared to other subgroups (p≤0.01, p≤0.01), however, it does not differ from the average sample percentage. Among individuals refused treatment for economic reasons, the Annual income value is significantly lower than in other subgroups and in the sample average (p≤0.01, p≤0.01, p≤0.01), and the percentage of expenses on AM drugs, on the contrary, is higher (p≤0.01, p≤0.01, p≤0.01). In the group of older patients indicated socio-economic reasons for the refusal of treatment (subgroup 3), the average score obtained in the evaluation of social functioning and role-emotional parameters was significantly lower than in other subgroups (p≤0.05 in all cases).
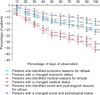
Fig. 1 illustrates change in the percentage of individuals refused treatment for a specific reason, and the percentage of individuals with altered objective characteristics of their status. The percentage of individuals indicated economic reasons for the refusal and those with altered economic status markers is statistically homogeneous. The percentage of individuals with impaired health status markers during 30% of the follow-up period was significantly lower than the percentage of patients indicated medical reasons for the refusal. The percentage of individuals with changes in social and psychological status markers during 60% of the follow-up period was statistically significantly higher than the percentage of individuals indicated social and psychological reasons for the refusal.
When analyzing the ratio of individuals having objective disturbance of any status to reasons for refusal indicated by the same individuals, we have revealed the following. Only 3 individuals (0.56%) among 554 patients with objectively impaired urodynamics (100%) indicated other than medical reasons for refusal. Ninety-seven point nine percent (97.9%) of 285 people with low economic status indicated economic problems as reasons for refusal of treatment. Every individual, who, according to our data, indicated psychological or social problems as reasons for refusal of treatment, had objective evidence of impaired social and psychological status. Thus, we have found no statistically significant difference between the number of individuals with objectively impaired parameters and the number of refusals for correspondent reasons in these same individuals.
DISCUSSION
During the experiment, we found that urge, urinary incontinence, Qaver, bladder volume values, as well as the percentage of patients with side effects in cohorts with different adherence were statistically nonhomogeneous. Values of economic status parameters—annual income, annual medical cost and expenses on AM drugs—were significantly different in patients with varying adherence as well. The average score in the evaluation of social functioning, role-emotional and role-physical differed significantly in cohorts with different adherence level.
The percentage of individuals indicated medical factors as reasons for the refusal of treatment during 30% of the follow-up period was significantly higher than the percentage of individuals whose health status parameters were altered objectively. The percentage of individuals indicated social and psychological reasons for the refusal during 70% of the experiment time was significantly lower than the percentage of individuals with the disturbance of objective social and psychological status markers. When analyzing data, we have found that individuals with objectively disturbed parameters usually reasonably state them as the reason for refusal of treatment. However, we have found a significant number of individuals with normal urodynamic parameters and high economic status, who indicated medical and economic reasons for refusal. On the contrary, a number of individuals having objective severe social and psychological problems had not indicated them as reasons to refuse treatment.
According to the literature, the percentage of treatment refusals associated with the lack of efficacy, side effects and pharmacological characteristics of different AM drugs exceeds 50%–65% and more [1218]. Other researchers report the absence of effect of the pharmacological differences between drugs on the long-term adherence [10], which, however, is not a common point of view and is often disputed [12]. In our study, only 36.5% of patients indicated medical reasons for the decision to discontinue the AM drug administration, and only 31.9% have the parameters of the lower urinary tract condition and the percentage of side effects differing significantly from the average sample values of these parameters. Perhaps to some extent these results can be explained by the lack of high expectations in older patients, long previous experience of OAB treatment, a habit of monotonous drug administration in polymorbidity.
Many authors indicate the need of taking into account the patients' economic status evaluating a rate of refusals for these reasons in 12%–19% and more [1819]. According to our data, not less than 20.2% of older patients indicate economic reasons for the refusal, while the change in objective economic status markers was observed in 16.4%, thus making both cohorts statistically homogenous, and confirming substantial significance of economic problems in motivating the refusal of treatment. Vecchioli et al. [30] based on the results of their observations, concluded that AM drugs' cost can have a direct influence on the patients' decision to discontinue treatment. Moreover, patients often do not indicate economic difficulties as the reason for their decision, which can lead an urologist to a wrong opinion about the drugs' efficacy.
It relates much more to, according to our data, psychological and social reasons for the refusal. In 13.2% of cases patients indicated these very reasons influencing on their negative decision, but according to objective data not less than 21.9% have psychological problems or a decreased level of social adaptation. Perhaps this is related to the lack of adequate self-analysis, to the resistance of the part of patients to recognizing social and psychological problems referring to, in their opinion, more “acceptable” reasons, such as “a mismatch between expectations and treatment results”.
The experiment protocol does not provide for the comparison of the adherence to AM drugs and other OAB treatments, a study of the adherence to treatment in other forms of urination disorders, a study of a number of economic characteristics. These and some other issues require further study.
Twenty-four patients (1.4%) discontinued their participation in the experiment for unrelated reasons (moving, death, diagnosis of diseases requiring urgent treatment with other anticholinergic drugs), in 28 cases (1.6%) it was not possible to collect comprehensive information on patients' income and expenses. 14 patients (0.8%) were not able to formulate a reason for the refusal of treatment.
CONCLUSIONS
We confirmed the results of other studies that long-term adherence to AM drugs treatment is poor – only 52.6% of the older take drugs of this class during 6 months, and 30.1% during the year. At the same time, according to our data, medical and health-related reasons have no dominant value in motivating older patients – they are referred to in 36.5% of cases of the refusal of treatment. 20.2% of patients refuse to continue treatment for economic reasons, 13.2% of patients for social and psychological reasons. However, the study of objective markers of patients' status first allowed to find out that a significant number of patients states incorrect information as reasons for the refusal: they indicate medical reasons for the refusal in objectively satisfactory health status markers, avoid indicating psychological and social problems as a motive for the refusal of treatment in poor social and psychological status.
The result of this experiment can be used in the urological practice for predicting results of the AM drug prescribing, evaluating risks of refusals of proposed therapy associated with motivations other than those indicated by patients themselves.



 XML Download
XML Download