

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Renal cell carcinoma (RCC) is the most common malignancy of the kidney and a cancer of increasing incidence [1]. In Korea, RCC accounted for 1.85% of the total cancer occurrence in 2012, and the incidence rate was 8.2 per 100,000 people [2]. The incidence of this cancer is relatively low among genitourinary malignancy, leading to the management of a lower volume of RCC cases in most hospitals. Therefore, it is difficult to make generalizations based on studies of RCC performed by single center due to the lower number of cases and the possibility of selection bias. Therefore, it is necessary to establish a well-qualified multi-institutional database (DB) system comprising a large cohort to conduct clinical RCC researches due to the lower incidence of this neoplasm. And this database should include more variable data than the cancer statistics of National Cancer Center or Health Insurance Review & Assessment service.
Some international groups have performed RCC studies based on multi-institutional RCC DBs. Examples include the renal mass study of CROES (Clinical Research Office of the Endourological Society) [34], CORONA (Collaborative Research On Renal Neoplasms Association) Project [5
6789], SATURN (Surveillance and Treatment Update Renal Neoplasms) Projects [89] and Japanese multicenter studies [1011], which have reported high-quality research results. Some multi-institutional retrospective studies on RCC have also been conducted in Korea [121314], but there have been no large DB systems to collect data on Korean RCC. Here, we report the establishment of the 1st Web-based RCC DB system in Korea (KOrean Renal Cell Carcinoma, KORCC) and summarize the basic characteristics of Korean patients with RCC who underwent surgical management.
Go to : 
MATERIALS AND METHODS
The new Web-based DB system was established to collect basic demographic and clinicopathological characteristics of a large cohort of patients with RCC in Korea. This project was approved by local ethics committee at Seoul National University Bundang Hospital (IRB number: B1202/145-102). The data included basic demographic (such as age, gender, height, and weight) and clinicopathological characteristics (such as clinical stage, perioperative parameters, pathological stage, Fuhrman nuclear grade and survival data) (Tables 1, 2, 3, 4, 5). AJCC cancer staging manual was used for TNM staging [15]. Private information (such as resident registration number and hospital ID number) was excluded to protect the patients' personal information.
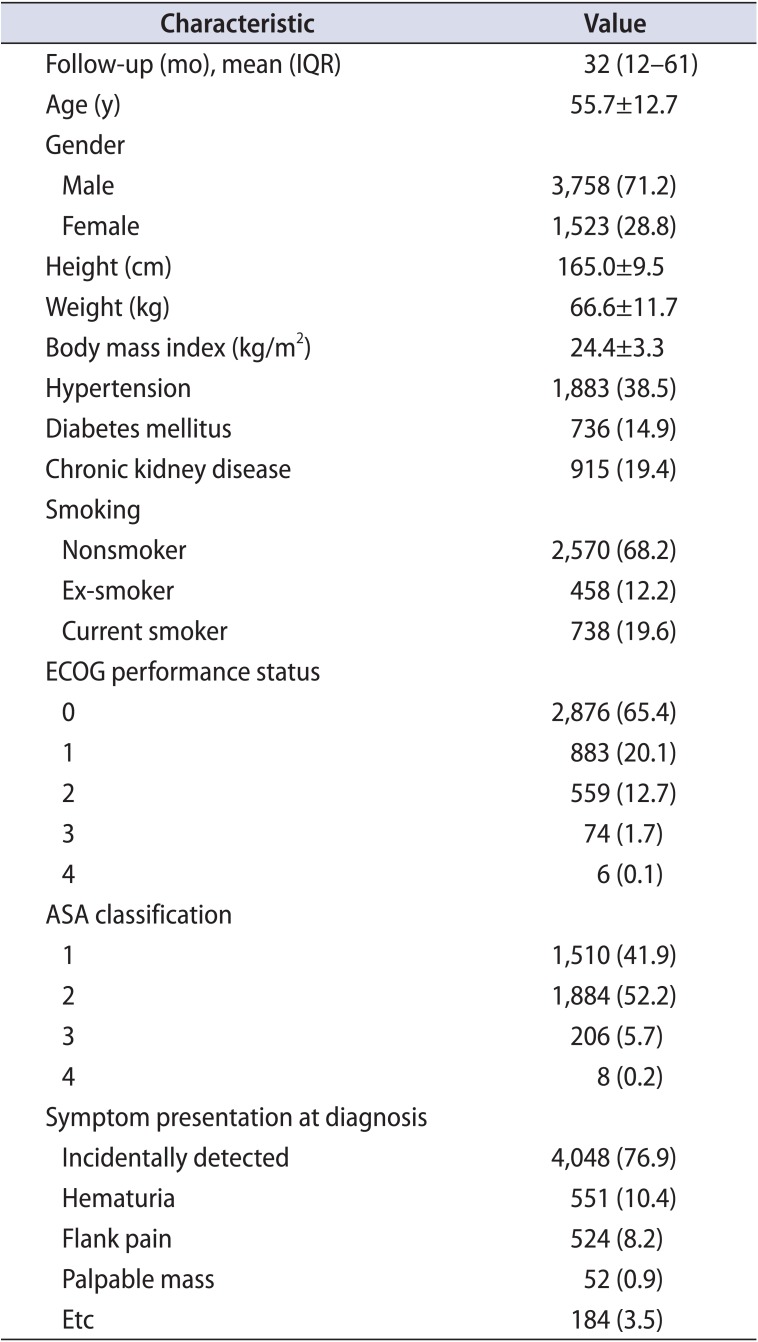
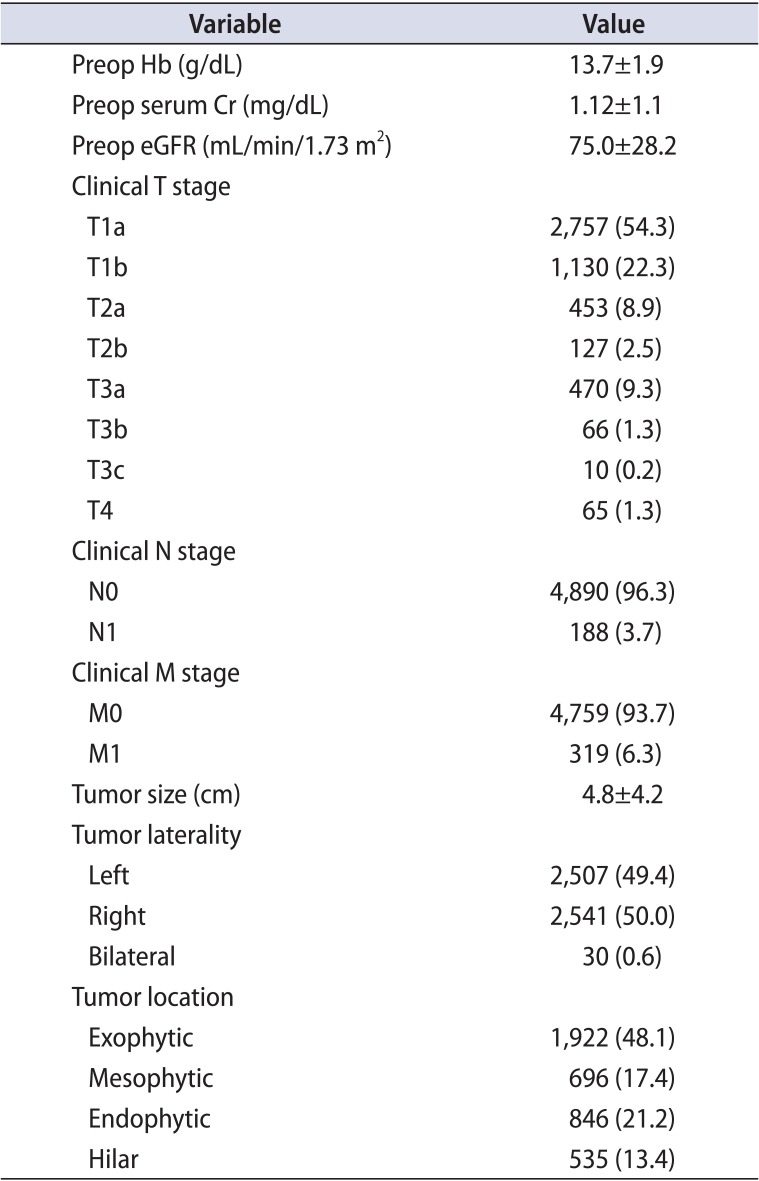
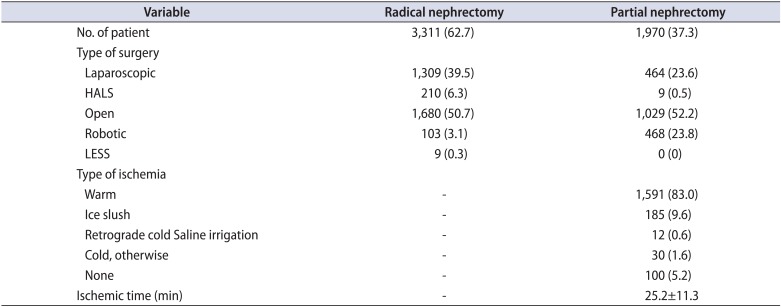
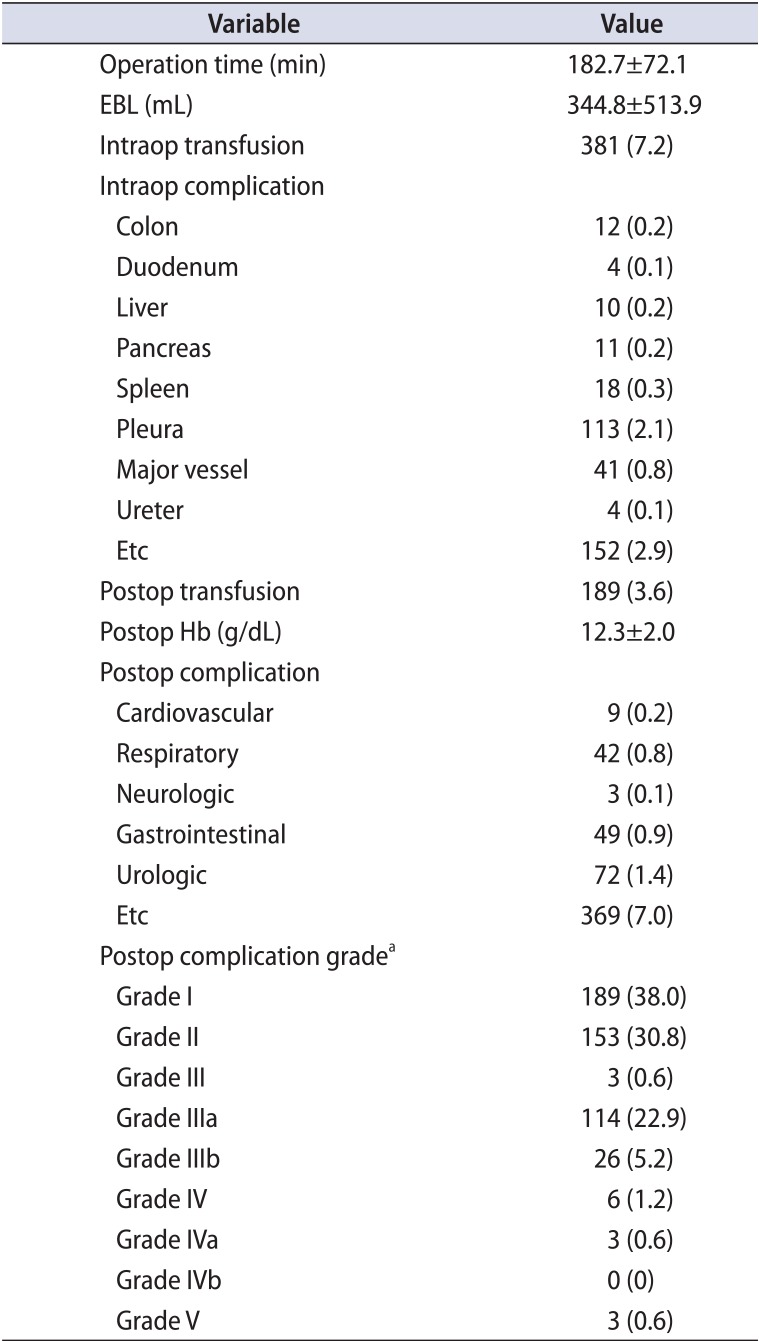
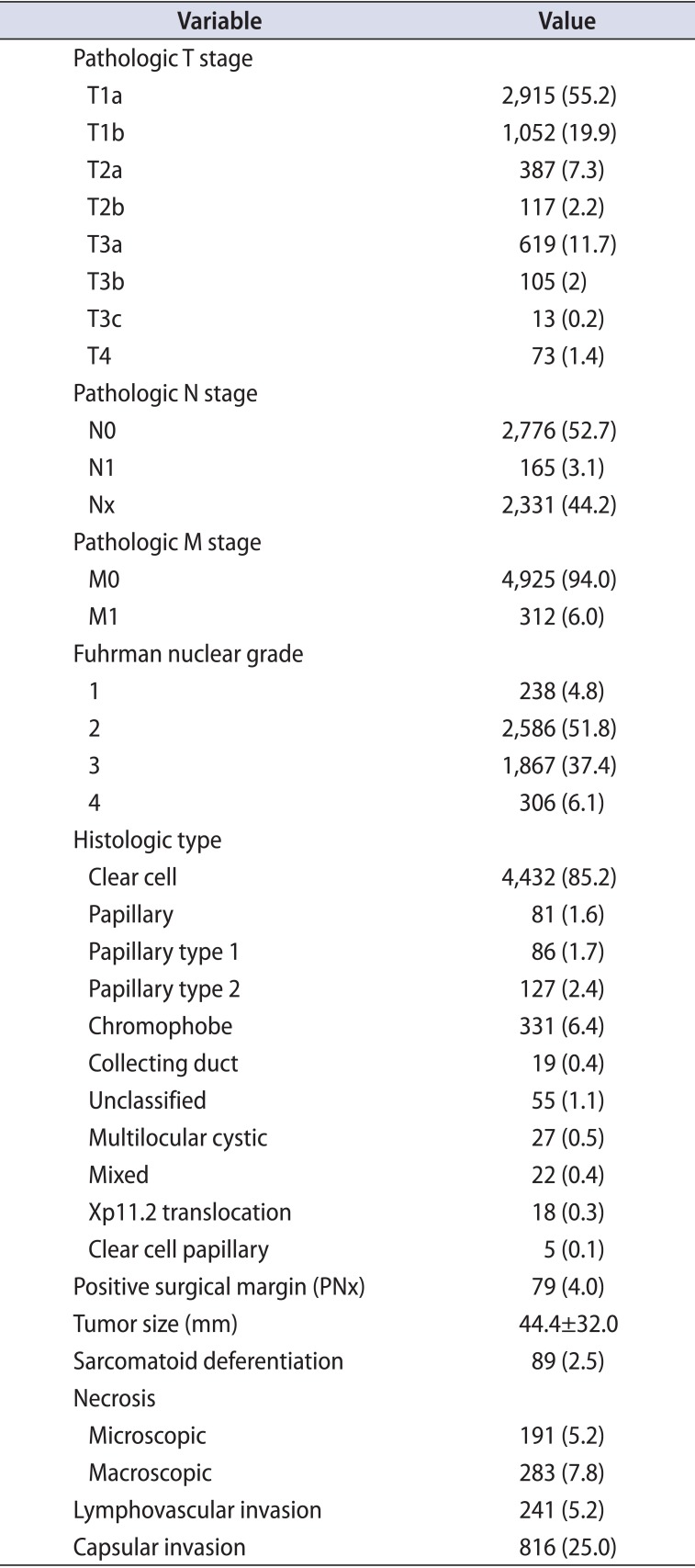
Table 1
Basic characteristics (n=5,281)
![]()
Table 2
Preoperative findings
![]()
Table 3
Type of surgery and ischemia
![]()
Table 4
Perioperative findings
![]()
Table 5
Pathologic characteristics
![]()
Data from a total of 6,849 patients were collected from 8 tertiary care hospitals that agreed to participate in organizing KORCC study group as of 1 July 2015. These hospitals were Chonnam National University Hwasun Hospital (308 cases), Chungbuk National University Hospital (178 cases), Korea University Anam Hospital (105 cases), Kyungpook University Medical Center (890 cases), National Cancer Center (618 cases), Seoul St. Mary's Hospital (883 cases), Seoul National University Bundang Hospital (1,440 cases) and Seoul National University Hospital (2,427 cases). Data were collected for the management of renal masses of all tumor stages (pT1-4, N0-2, M0-1) at the Department of Urology at each hospital from 1990 to present (time frame varies among hospitals due to differences in their own DB collections). Hospitals have contributed to the database by adding all consecutive patients until now.
We analyzed the data of patients who underwent surgical treatments. They were compared with those of previous international studies to characterize Korean RCC. Some data were excluded from the analysis due to insufficient or missing variables.
Go to :
RESULTS
We established the 1st Web-based DB of KORCC, a database comprising renal mass management cases from multiple centers in Korea (www.mebica.net). A total of 6,849 patients were collected nationwide from 8 tertiary care hospitals in Korea.
We analyzed data of 5,281 patients with surgical management (mean follow-up [FU], 32 months) (Tables 1, 2, 3, 4, 5). The patients' mean age was 55.7±12.7 years, and 71.2% of the patients were male (Fig. 1). Hypertension, diabetes mellitus and chronic kidney disease (defined as grade 3 or more) were identified in 38.5%, 14.9%, and 19.4% of the patients, respectively. The most common symptom was incidentally detected renal mass (4,048 cases, 76.9%), and the 2nd most common was gross hematuria, which accounted for 10.4%.
Preoperative characteristics-such as clinical stage, tumor size, laterality, and location-were described in Table 2. Clinical T1a was the most common (54.3%) stage, and the mean tumor size was 4.8±4.2 cm.
Radical nephrectomy accounted for 62.7% of the total cases, and an open approach was used in 50.7% and 52.2% of radical and partial nephrectomies, respectively (Table 3). Warm ischemia was the most common type of ischemia (83.0%) and mean ischemic time was 25.2±11.3 minutes.
Intraoperative and postoperative transfusions were done in 7.2% and 3.6% of the patients, respectively (Table 4). Intraoperative and postoperative complications occurred in 6.9% and 10.3% of the patients, respectively. A total of 2.9% of severe postoperative complications were of Clavien-Dindo grade ≥3 [16].
Pathological characteristics are shown in Table 5. T1a accounted for 55.2% of the total cases. The most common nuclear grade was Fuhrman grade 2 (51.8%) and the most common histological type was clear cell (85.2%). Positive surgical margins were identified in 4.0% of the patients undergoing partial nephrectomy.
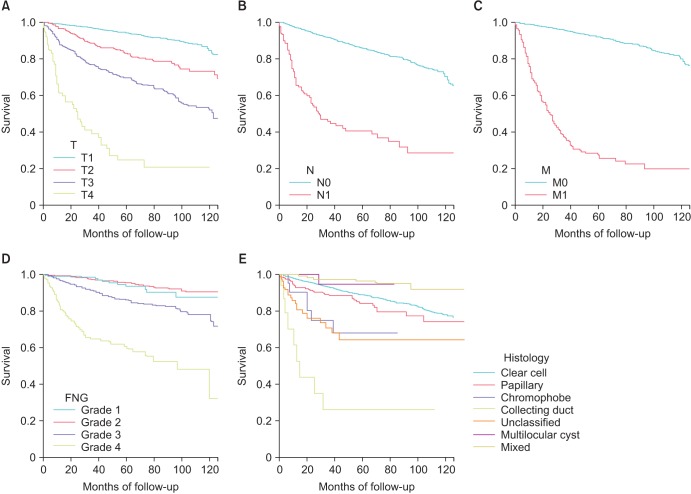
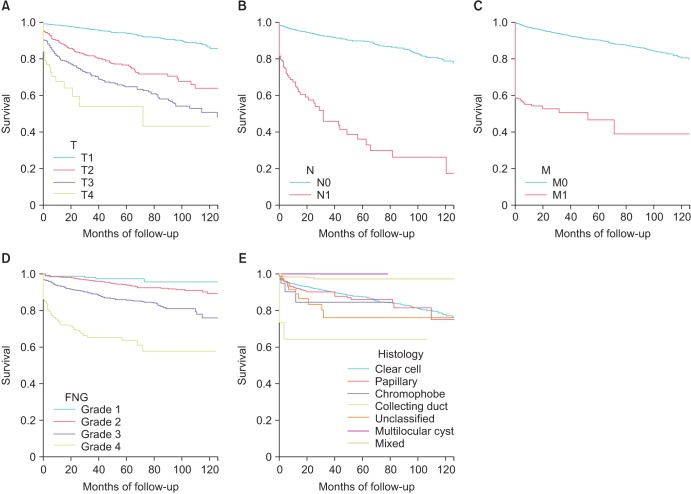
The 5-year overall, cancer-specific and recurrence-free survival rates were 88.1%, 92.2%, and 88.0%, respectively (Table 6). Kaplan-Meier survival curves according to stage, nuclear grade and histologic type are shown in Figs. 1, 2.

Go to :
DISCUSSION
We report the 1st establishment of a Web-based DB system to collect clinicopathological characteristics of RCC in Korea. This project was initiated with the aid of 5 participating centers in 2011. The KORCC Web-based DB system was launched in 2013, finally leading to the participation of 8 centers nationwide in 2014. There are already some publications through the use of this DB [141718]. It is necessary to collect data from a large cohort of RCC patients to provide better analysis of RCC data in Korea. Data from approximately 7,000 RCC cases were collected, and this project remains ongoing to collect more cases. We believe that this DB can represent Korean RCC due to its large cohort size and nationwide distribution.
Several factors were of concern in the establishment of this system. First, we aimed to collect data that was representative of Korean RCC. Therefore, we invited 8 nationwide tertiary care centers to participate in this project, and they all agreed to join. This led to the creation of a DB that represents RCC characteristics of Korean patients. Second, because this system is Web-based, there is possibility that patients' data could be leaked due to security problems. Therefore, we chose an experienced company that has built many Web-based clinical trial DB systems (Mebixon Co., Seoul, Korea). Personal information-such as resident registration number and hospital identification number-was not included in our DB system. This led to the establishment of a secure Web-based DB system of RCC in Korea.
For the good quality of this database, we limited the number of hospital as above. In the future, if the database works well, we will invite other hospitals to participate in KORCC and provide chances to investigate with this database.
There have been many multicenter based studies on RCC, and CROES was the 1st group to establish an international electronic data management system [3]. The global renal mass study driven by CROES was started in 2008 to provide a prospective international study on the indications, treatment modalities and outcomes of the management of renal masses. Each center participating in this project included all of the patients with the diagnosis of renal mass during a one-year period. Other examples of international multi-center collections were the CORONA and SATURN projects [56789], which were not Web-based. Nevertheless, this type of multicenter collection is necessary to obtain better knowledge on RCC through a DB with a large cohort.
Data from 5,281 patients who underwent radical or partial nephrectomy were analyzed. Interestingly, incidentally detected renal mass accounted for 76.9% of the total patients. This rate was much higher than the rate of approximately 50% in a previous report [19]. Recently, the more common applications of imaging modalities for the evaluation of a variety of nonspecific symptoms has led to higher rates of incidental mass detection and an increased proportion of early stage tumors. More than half of the patients (54.3%) presented with clinical T1a stage tumors and metastatic tumors were identified only in 6.3% of patients. It is probable that this rate overestimated the real pattern of presentation because patients with advanced stage disease who were managed by hematooncologic department were not included in our DB system. This relatively higher proportion of low clinical stage contributed to excellent overall and cancer-specific survival rates. We will likely find more incidental tumors with lower stages with the increasing use of imaging studies in the future.
Nowadays, the use of minimally invasive surgery is a growing trend. An open approach was used in 50.7% and 52.2% of radical and partial nephrectomies, respectively. Minimally invasive approaches-such as laparoscopic and robotic surgeries-were used for the remaining cases. Interestingly, robotic approach was used in 3.1% and 23.8% of radical and partial nephrectomies, respectively. It is well known that the application of robotic surgery in partial nephrectomy can provide good surgical quality including a reduced ischemic time, due to its enhanced 3-dimensional vision and excellent degree of freedom [2021]. These factors contributed to nearly a quarter of the patients undergoing partial nephrectomy being managed by a robotic approach. Although it represented a relatively lower (3.1%) proportion, robotic technology was also used in radical nephrectomy. Pure laparoscopic surgery is a challenging procedure, and some surgeons find laparoscopic radical nephrectomy difficult to perform. Robotic radical nephrectomy can bridge the gap between open and pure laparoscopic approaches for some urologists. As the number of people with private insurance has increased and the cost barrier is not an issue for these patients, the application of robotic technology will continuously increase in the future.
Another notable f inding was that proportion of clear cell type was higher (85.2%) in our DB compared to that in previous reports (60%-80%) [2223]. Whether this phenomenon is Korean-specific is not known. The proportion of sarcomatoid differentiation has ranged from 2% to 5% in past reports; our DB revealed a proportion of 2.5%, which was equivalent to other reports [2425].
There were some limitations in this DB. First, this type of retrospective collections could contain some errors in data entry. We crosschecked our data with alternate recorders to avoid some errors in data entry. In addition to this error, some patients' data were lacking, causing incomplete data collections for some individual patients. Second, the length of FU length was rather short (mean, 32 months) but this weak point will be solved with long-term FU in the future. Third, this collection was based on the department of urology at each center. Some patients with advanced stage disease could visit the department of internal medicine and they could be managed without surgical intervention. This could lead to incomplete observation of the whole RCC spectrum in Korea. We are planning to expand this database to include patients of hematooncologic department. Then, the database will be able to represent the whole cohorts of Korean RCC.
In conclusion, the 1st Web-based DB system to collect RCC data was established in Korea. This DB will provide a solid basis for the characterization of KORCC.
Go to :
 XML Download
XML Download