

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bladder is the most common site in the urinary system to be afflicted by cancer [1]. At presentation, approximately 30% of bladder cancers (BCa) are muscle invasive [2]; radical cystectomy (RC) remains the treatment of choice in these cases [3]. However, in select patients, partial cystectomy (PC) may offer equivalent oncological control with superior quality-of-life [4].
PC, when indicated, has most commonly been performed via an open-approach as it permits gross evaluation of the excised specimen and intraoperative assessment of surgical margins. However, techniques of laparoscopic PC (LPC) with or without robotic-assistance have been described [56789]. Colombo et al. [7] reported on 6 cases of LPC for bladder or urachal malignancy. Tareen et al. [8] and Allaparthi et al. [9] reported on 4 and 3 cases of robot-assisted PC (RAPC), respectively, establishing the feasibility of RAPC in management of bladder neoplasms.
Although, performing PC minimally-invasively may reduce the morbidity of the procedure there is a theoretical risk of inadequate surgical resection that has not been addressed in these previous reports. Accordingly, in the current study, we sought to test the feasibility, safety, and reproducibility of a novel 'modification' of RAPC that recapitulates the open technique and allows for intraoperative surgical margin assessment. Further, we report on perioperative, oncological, functional, and quality-of-life outcomes in patients undergoing RAPC.
MATERIALS AND METHODS
1. Patient cohort
Between 2008 and 2013, 7 patients consented to undergo RAPC, with the latter 5 undergoing modified-RAPC (m-RAPC) using the GelPOINT device (Applied Medical, Rancho Santa Margarita, CA, USA). We have previously demonstrated the efficacy of this technical modification in assessing and reducing positive surgical margins (PSMs) during robotic radical prostatectomy and robotic partial nephrectomy [1011]. In the current study, we extend the same principle to the management of BCa.
2. Covariates
For each patient age at surgery, sex, body mass index (BMI), history of abdominal surgery, risk factors for BCa, tumor characteristics [12], neo-adjuvant therapy and operative details were recorded.
3. Outcomes and regret and satisfaction survey
Perioperative outcomes evaluated included surgery times, blood loss, surgical margins, hospital stay and complications. Disease recurrence and survival endpoints were also assessed, with a minimum and median follow-up of 12 and 38.9 months, respectively. Lastly, at the time of the last follow-up patients were surveyed to assess regret and satisfaction with treatment using previously validated questionnaires [1314]. Regret was assessed by the following 3 questions: (1) The man/woman's wish that he/she could change his/her mind about the kind of treatment he/she had received; (2) His/her feeling that he/she would be better if he/she had chosen another treatment; (3) Whether he/she was bothered by the fact that others received different treatment for their BCa (the responses were: "none of the time," "a little of the time," "some of the time," "most of the time" or "all of the time" - No regret was defined as "none or a little of the time"). Satisfaction was assessed by the following 3 questions: (1) How would you rate your overall satisfaction with your treatment choice?; (2) How would you rate your satisfaction with regards to urinary control?; (3) How would you rate your satisfaction with regards to cancer control? (the responses were: "extremely satisfied," "satisfied," "unsure," "dissatisfied" or "extremely dissatisfied" - Satisfaction was defined as "extremely satisfied or satisfied").
4. Surgical technique
In the 5 patients undergoing m-RAPC, the GelPOINT device allowed for rapid specimen extraction without compromising the pneumoperitoneum. After induction of general anesthesia, the patient was placed in supine position and the GelPOINT access port was inserted supraumbilically through a 4- to 5-cm vertical incision. Next, the GelSeal cap, prepared with a 12-mm camera port and a 10-mm low profile port (Fig. 1A), was secured on-top of the GelPOINT access port. Linear incisions were made in the GelSeal at a tangent to the 10-mm port on the GelSeal cap to facilitate specimen retrieval postextirpation. Pneumoperitoneum at 20 mmHg was established. The patient was then placed in steep Trendelenburg and 5 additional trocars were inserted under direct vision. Two 8-mm robotic ports for the left and right robotic arms were inserted along the left and right paramedian lines at the level of the umbilicus, respectively. A 12-mm assistant port was inserted near the right iliac-fossa along the anterior axillary line, and two 5-mm assistant ports were placed; one for suction in the epigastrium between the GelPOINT and the right robotic port, and the other for the left side assistant in the left iliac fossa (Fig. 1B). Subsequently, the robot was docked in the side-dock position, along the left foot end, to permit intraoperative cystoscopy.
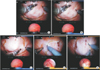
Robotic instruments included a fenestrated bipolar grasper in the nondominant hand and monopolar curved scissors in the dominant hand; the latter instrument was exchanged for a robotic needle driver during reconstruction. Depending on tumor location (Table 1), the bladder exposure varied. For cases in which the tumor was located at the dome or the anterior wall of the bladder, the bladder was taken down caudally up to the level of the endopelvic fascia freeing the pedicle lateral to the umbilical ligament. In cases where the tumor was located at the lateral wall or near the ureteral orifice, the procedure began with medialization of the sigmoid colon followed by identification of the ureter at the iliac vessel crossing. The ureter was then traced caudally to the level of the bladder. The vas deferens or round ligament was divided as needed. Next, the bladder was filled with normal saline and a flexible cystoscope was introduced for intraoperative tumor localization (Fig. 2A, B). A robotic ultrasound-probe (BK Medical, Peabody, MA, USA), passed through the 12-mm assistant port, was also utilized for tumor localization in 2 cases allowing for further confirmation and precise localization of the tumor within the bladder (Fig. 3A, B). When tumor location necessitated vascular pedicle control, this was achieved with hem-o-lock clips, and the superior vesical and inferior vesical arteries were clipped and ligated in succession. Following this, using cystoscopic assistance, with or without the robotic ultrasound-probe, the margins of the tumor were delineated and the detrusor muscle was scored circumferentially to achieve a 10- to 20-mm margin (Fig. 4A–E). The bladder was then drained and the detrusor muscle was transected. The bladder mucosa was then entered and the tumor was excised circumferentially without energy. After excision, the tumor was placed in an Endo-Catch bag (Ethicon Surgery Inc., Cincinnati, OH, USA) and brought up through the GelPOINT (Fig. 5A). Three steps were routinely performed to reduce the potential seeding of the abdominal cavity by cancerous cells; first, the bladder was drained before entering the mucosa, second, the incised area was held up (with the help of stay sutures) until the defect was sutured closed, and lastly, the excised specimen was captured and placed directly into an Endo-Catch bag without allowing it to touch/rest on adjacent tissue.
Immediately following excision and extraction of the specimen, the surgeon examined the specimen on-table (Fig. 5B). Frozen-sections were taken from areas that appeared suspicious for a PSM on direct visualization and palpation (Fig. 5C), and after being carefully marked for anatomical orientation, were sent for frozen-section analysis (Table 2). If frozen-section yielded unfavorable pathology, more tissue was excised from the in situ complementary site and sent for permanent section. The bladder was then closed in 2 layers using a 3-0 barbed suture and left to closed drainage. Pelvic lymphadenectomy was performed as described previously [15]. The robot was then undocked and the fascia and the skin were closed in a standard manner. Post operative cystography was performed on all patients on postoperative day 7 prior to Foley catheter removal.
RESULTS
Table 1 provides data on patient demographics and preoperative characteristics. The mean age was 72.5 years; 71.4% of the patients were men (n=5). The mean BMI was 31.3 kg/m2. All patients underwent RAPC for a malignant indication.
Perioperative and follow-up data are detailed in Table 2. The overall mean operative and console times were 291 and 217 minutes, respectively. Mean estimated blood loss was 66.3 mL. No patient had a PSM; a potential PSM was prevented (case 6) by virtue of m-RAPC, as a positive intraoperative frozen-section lead to further tissue excision from the complementary site on the bladder, with subsequent negative surgical margin (NSM) (on the outer side) on final pathology. Mean length-of-stay was 1.7 days. One patient developed lymphocele postoperatively requiring drainage (Clavien-Dindo grade IIIa).
At a median follow-up of 38.9 months, all patients but one were recurrence free. This patient (case 6) was a high-risk patient who had developed BCa secondary to Cyclophosphamide therapy for skin lymphoma, and presented with high-grade multiple urothelial carcinomas (UCs) clustered together at the dome (Table 1). He developed a superficial recurrence 6 months postsurgery and was managed successfully with transurethral resection of the bladder tumor. He was tumor free at 9-month cystoscopy but had a recurrence again at 12 months. He died the subsequent week from an unrelated condition (Lewy-body disease).
The response rate for the regret and satisfaction survey was 100%. Zero percent of the patients expressed regret and 0% expressed dissatisfaction (in all 3 domains for both the questions). None of the patients had any lower urinary tract symptoms (Table 2).
DISCUSSION
As the incidence of BCa continues to rise in the United States and worldwide, PC has gained attention as a potential treatment option for selected patients with muscle invasive BCa [1].
To decrease the burden of surgical morbidity, a minimally-invasive approach to PC has been suggested. Ferzli et al. [5] reported the first case of minimally-invasive PC in a female patient, establishing its feasibility. Mariano et al followed suit and reported a case series of 6 patients diagnosed with UC undergoing LPC, with only a single case of recurrence at a median follow-up of 30 months [6]. Colombo et al. [7] in their series on LPC further established its safety but highlighted that the technical demands of the procedure may limit its adoption. More recently, Tareen et al. [8] and Allaparthi et al. [9] successfully demonstrated the applicability of the robotic-approach to LPC. Tareen et al. [8] reported primarily on the utility of RAPC in management of benign bladder neoplasms (3 out of 4 cases) while all 3 patients in study by Allaparthi et al. [9] underwent RAPC for a malignant indication. In our study also, all 7 patients underwent RAPC for a malignant indication and we believe this represents the largest experience of RAPC in patients with cancer of the bladder.
The biggest drawback of RAPC, to date, has been the inability to retrieve tissue specimens prior to undocking the robot. Intraoperative tissue evaluation is important as it allows the surgeon to inspect the specimen margins grossly as well as send tissue for preliminary pathology review ensuring NSMs. The significance of achieving NSMs was demonstrated by Ashley et al. [16] in their study of 130 patients undergoing PC; the authors noted that in multivariable analysis, NSM was one of only 2 predictors that were significantly associated with improved survival. The m-RAPC technique overcomes the aforementioned drawback of standard-RAPC, and provides the surgeon with the ability to extract the specimen without undocking the robot and send tissue for frozen-section analysis during cystorrhaphy/pelvic lymphadenectomy. By performing cystorrhaphy/pelvic lymphadenectomy while waiting for the results of frozen-section analysis allows the procedure to be completed in a timely fashion. Accordingly, we did not note any increase in operative (p=0.67) or console time (p=0.81) for the five m-RAPC cases as compared to the 2 standard RAPC cases (Table 2).
Further, all seven patients had favorable perioperative outcomes including minimal blood loss, 1- to 2-day hospital stay, unremarkable cystograms and negative tissue margins. Long-term oncological outcomes were also favorable with only 1 patient experiencing a superficial recurrence at a median follow-up of 38.9 months, corroborating previous findings [46].
Lastly, we show that patients undergoing RAPC have excellent functional outcomes and quality-of-life (Table 2), which to the best of our knowledge has not been reported before for PC patients. The issue of satisfaction and regret becomes important when several potentially equally-efficacious choices exist for management of a particular disease; in such scenarios, clear portrayal of risk and benefits of each approach and involving patient in the decision making process might lead to higher patient satisfaction and lower regret post-therapy [1314]. This is demonstrated in our study by example of patient 6, as despite having an early recurrence, the patient expressed no regret or dissatisfaction.
Despite its merits, our study is not devoid of limitations. First, the study represents a retrospective review of prospectively collected data and thus is subject to the biases inherent to retrospective study designs [17]. Second, the regret and satisfaction survey results were not obtained at a constant time-interval from the date of surgery for each patient, which might have confounded the survey results [18]. Lastly, the sample size is limited. However, this study was done with the aim of testing the feasibility and safety of our new modification to RAPC and reporting the early outcomes in the initial patients.
Nonetheless, keeping in mind these drawbacks and in an effort to overcome them, we hope to pursue a prospective development study (IDEAL phase 2a study) in the near future following the IDEAL (idea, development, exploration, assessment and long-term monitoring) guidelines of surgical innovation proposed by the Balliol Collaboration [192021].






 XML Download
XML Download