

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Testicular germ cell tumors comprise the most common group of solid malignancies in male population of 15 to 35 years old. These tumors account for approximately 95% of all testes cancers [1]. The incidence of testicular tumors varies in different countries and ethnic groups with the highest reported incidence in Scandinavia region (about 9 in 100,000 males) [23]. Few reports are present about the incidence and epidemiologic features of testis cancer in the male population of Asian and Latin American countries, which indicate that testicular germ cell tumors are less common in these regions than most western countries [2]. A recent study has shown that the incidence of testis cancer is 1.3 in 100,000 male population in Iran [4].
Several risk factors contribute to testicular cancer. These include positive family or personal history of testis tumor, cryptorchidism and intratubular germ cell neoplasia (ITGCN). ITGCN was first described by Skakkebaek as carcinoma in situ of testis [56]. The nomenclature, carcinoma in situ was later replaced by ITGCN.
ITGCN is a precursor to almost all types of testicular germ cell tumors. Earlier studies have claimed that concomitant ITGCN is seen in 80%–90% of testes affected by germ cell tumors using immunohistochemistry (IHC) [67]. Progression risk of ITGCN to malignant germ cell tumors is 50% for 5 years and 70% for 7 years [7]. Thus, ITGCN is also considered as a premalignant lesion and prompt treatment is essential if it is incidentally discovered in testis biopsy. In addition, in cases of testis sparing surgery, ITGCN may be observed in the remnant tissue. In these situations, treatment of ITGCN is also necessary [8].
In the present study, we aimed to assess the prevalence of ITGCN in the patients who have underwent radical orchiectomy due to testicular tumor, as well as its correlations with pathologic features of concomitant testis cancer and patients' epidemiologic characteristics. To our knowledge, this is the first report on ITGCN in association with testicular germ cell tumor in our region, also the first study which is looking for its prognostic role.
MATERIALS AND METHODS
This is a descriptive – analytical and cross sectional study which was performed in our center. The study population was the patients who underwent radical orchiectomy due to testis tumor from 2003 to 2015. A total of 179 patients were identified with testis tumor. All patients had undergone radical orchiectomy via inguinal approach. Serum tumor markers had been measured before the surgery and consisted of alpha-fetoprotein (α-FP), and beta-human chorionic gonadotropin (β-HCG).
CD-117 (c-kit) and placental-like alkaline phosphatase were two immuno-reactive agents that were used to identify ITGCN via IHC [9]. Data about patients' age at the time of surgery, predisposing factors (such as family history, cryptorchidism), testis atrophy, and serum tumor marker before surgery were recorded and gathered for further analysis. Ultrasound characteristics and histologic reports were also gathered and classified. Pathologic reports were categorized as pure seminoma, mixed germ cell tumors (MGCTs; defined as containing at least two pathological subtypes of germ cell tumors), pure mature teratoma, embryonal carcinoma, yolk sac tumor, lymphoma and benign lesions (Leydig or sertoli cell tumor) [910]. One expert pathologist reviewed the specimens using light microscopy and IHC reports.
Data was gathered and analyzed using IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA). Descriptive criteria and prevalence of ITGCN were determined. Independent sample t-test was obtained to assess any relationship between ITGCN and quantitative factors. For qualitative factors we used chi-square test and Fisher exact test as needed. A p-value less than 0.05 was considered as significant. The Institutional Review Board of Iranian Urology and Nephrology Research Center approved the study design.
RESULTS
Mean age of the patients was 34.5 years old (range, 1–82 years). Eighty-four point four percent (84.4%) of patients (n=151) were in the range of 20 to 50 years and 2.2% (n=4) were under 12 months old.
Twelve patients had history of cryptorchidism (6.7%). History of testis atrophy (confirmed by ultrasound study) was observed in 8 cases (4.5%). Right and left testicles were involved by tumor in 96 and 83 cases, respectively. No cases of bilateral testicular tumor were seen. Calcification (diagnosed by ultrasound study) was observed in 87 patients (48.6%).
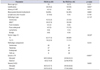
Pathologic reports showed that pure classic seminoma and MGCTs were the most common histologic types. Mean testicular parenchymal involvement was 54.3%. Considering the pathologic components of all cases (including those with MGCT), we found that seminoma was also the most prevalent component. Lympho-vascular invasion was seen in 12 patients (6.7%). Pathologic features of the patients are demonstrated in Table 1.
While primary study of the specimens by light microscopy leaded to diagnosis of ITGCN in only 21 patients (11.7%), further analysis by IHC staining increased this figure to 85 patients (47.5%). So, it seems that light microscopy missed about three-fourths (75%) of patients with ITGCN. With exclusion of lymphoma and benign lesions, the prevalence of concomitant ITGCN was determined as 49.4%. The correlation of ITGCN with epidemiologic and pathologic factors is summarized in Table 2. There was not a statistically significant difference in mean age, histologic type, histologic components, cryptorchidism, and lymphovascular invasion between the 2 groups (p=0.151, p=0.11, p=0.233, p=0.413, and p=0.14, respectively). However, calcif ication of testis parenchyma, as identif ied by ultrasonography, was lower in patients who had concurrent ITGCN (35% vs. 59%, p=0.001).
The prevalence of ITGCN was significantly lower in the patients with stage T1 than those with higher stages (≥T2). Among the 150 patients with stage T1, 62 (41%) had ITGCN, while 18 out of 29 patients (62%) with stage T2 and T3 had ITGCN (p=0.03).
Since patients with pure seminoma do not present with elevated serum tumor markers, any relationship between ITGCN and tumor markers was assessed in 98 patients with nonseminoma histology. Fifty-two patients with nonseminoma pathology had concomitant ITGCN, of which 44 patients (84.6%) had elevated serum α-FP before the surgery, while in the other group, only 24 patients (52%) had elevated serum α-FP level. Thus, elevated serum α-FP level is much common in patients with ITGCN (p<0.001). Prevalence of elevated serum β-HCG was 58% and 64% in patients with and without ITGCN, respectively; which did not indicate a significant difference (p=0.6).
DISCUSSION
Testicular germ cell tumors are the most common solid tumors in young men. There are several risk factors that contribute to testis cancer, including family or personal history, cryptorchidism, and ITGCN [1]. Skakkebaek [6] have noticed that almost all types of testicular germ cell tumors (except germ cell tumors in children and spermatocytic seminomas) originate from ITGCN. They are typically larger than normal spermatogonia, with prominent nuclei and abundant cytoplasm. They lie in seminiferous tubules in a single row just like normal cells. The microscopic features of ITGCN resemble that of seminoma and IHC is needed for exact diagnosis [11]. The results of our study shows that light microscopy might underestimate ITGCN in patients with testicular germ cell tumors.
The incidence of testis cancer varies according to different regions and ethnic groups. It is higher in Western countries and Scandinavia region, and lower in African Americans and Asian countries [1213]. The incidence of testicular cancer is about 5.3 cases per 100,000 in the United States [14], but the highest rate of testis cancer has been reported from Scandinavia region as about 9 in 100,000 [23]. Several studies have shown that the incidence of testicular germ cell tumors is increasing [1516].
A recent study by Basiri et al. [4] has shown that the incidence of testis cancer is lower in Iran than Western countries. In 2009, the incidence of testis cancer in Iran was reported as 1.3 in 100,000. The reason for this difference is not yet clarified. Since ITGCN is a major risk factor and precursor to most testicular cancers, we decided to evaluate the prevalence of ITGCN and its correlations with other histologic factors in an Iranian population who had testis tumor.
Earlier studies by Skakkebaek [617] and Montironi [7] indicated that 80%–90% of patients who undergo radical orchiectomy have simultaneous ITGCN in the adjacent tissue. Another study by Klein et al. [18] have shown that 82% of seminomas and 75% of nonseminomas are associated with ITGCN. Our study revealed that Iranian patients trend to have lower incidence of ITGCN. This finding may be attributed to the low incidence of testis cancer in Iran. Using IHC, we found out that 47.5% of patients had concomitant ITGCN.
Although mean age of patients was lower in ITGCN group (32.6 years old), it was not significantly different from the overall group. Most previous studies showed a significant association between seminoma and ITGCN. The reason may be that both ITGCN and seminomas both originate from primordial germ cells (gonocytes) [910]. However, in our study only 56.7% of seminomas had concomitant ITGCN. The prevalence of ITGCN was not significantly different in various tumor subtypes.
Current data in the literature supports the idea that microlithiasis is not an independent predisposing factor for testicular cancer, although it may accompany other possible premalignant features [19]. A study by Meissner et al. [20] concluded that microlithiasis may be accompanied by ITGCN, and thus, healthy patients with several risk factors who present with microlithiasis need to undergo routine testicular biopsy to rule out ITGCN or testis tumor. This study and other previous surveys, evaluated the significance of microlithiasis and its correlation with ITGCN in healthy patients who did not have testis cancer at the time. However, the results of our study indicate that in patients who suffer from testis cancer, microlithiasis does not accompany ITGCN. In support of this idea, a recent literature review revealed that there are 5 conditions in relation to microlithiasis and testicular cancer: Down syndrome, McCune-Albright syndrome, cryptorchidism, infertility and familial disposition of testicular cancer. ITGCN was not reported to have a correlation to microlithiasis [21].
ITGCN was much common in patients with higher tumor stage (i.e., T2, T3). This may indicate that ITGCN is related with more aggressive tumors, which is a new finding. In addition, in patients with nonseminoma germ cell tumors, elevated serum α-FP level was closely related to ITGCN. More than 84% of patients with ITGCN had high serum levels of α-FP before orchiectomy.
This study was the first to evaluate the associations of ITGCN with epidemiologic and pathologic factors of testis cancer. High volume, multi center studies with larger sample size are needed to get more constant and reliable information about ITGCN.
CONCLUSIONS
The prevalence of concomitant ITGCN in the Iranian population who undergo radical orchiectomy is lower than most western countries. ITGCN is more common in higher tumor stages and is accompanied with elevated serum α-FP levels before the surgery. Since the prevalence of ITGCN is higher in the regions with high incidence of testis cancer and in high stages of germ cell tumors, presence of ITGCN in adjacent tissue may suggest a negative cancer behavior.

 XML Download
XML Download