

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In 2012, prostate cancer was the fifth most commonly diagnosed malignancy in Korean men, with an estimated 9,258 new cases detected annually [1]. Nearly 50,000 Korean men are living with prostate cancer, of whom 1,460 die from the disease each year [1]. Compared with Western countries, prostate cancer is less common in Korea (and in Asian countries in general) [2], although its prevalence doubled between 2002 and 2007, likely due to demographic aging, changes in diet, and increased prostate-specific antigen (PSA) screening [34567]. For example, a retrospective analysis of prostate cancer patient data collected between 2006 and 2010 from a tertiary care center (Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea) revealed a steady increase in the prevalence of prostate cancer, with 21% of patients reporting advanced or castration-resistant prostate cancer (CRPC) in 2010 [5].
As prostate cancer progresses metastases develop, and most cases respond to androgen deprivation therapy (ADT), at least initially [8]. Unfortunately, resistance to ADT always ensues, resulting in a transition to metastatic CRPC (mCRPC) [891011], a lethal clinical state defined by cancer progression despite effective lowering of serum testosterone to <50 ng/dL or 1.7 nmol/L [12]. Use of docetaxel plus prednisone is the current standard of care for mCRPC in Korea [1314], but this regimen is associated with toxicity and, ultimately, drug resistance [1415]. Recent evidence has highlighted the ongoing, central role of androgen receptor (AR) signaling in CRPC, suggesting that further inhibition of this pathway with noncytotoxic therapies may confer a survival benefit. Firstly, affected patients often have elevated serum PSA levels and measurable intratumoral androgens despite castrate levels of testosterone [16]. Secondly, preclinical data showed that AR overexpression is sufficient to confer resistance to ADT in prostate cancer cell lines [1718].
Enzalutamide is an AR inhibitor that has shown an 8-fold greater affinity for the AR than bicalutamide in studies of LNCaP/AR cells (half maximal inhibitory concentration, 21 nM vs. 160 nM) [19]. Enzalutamide also has the capacity to reduce the efficiency of AR nuclear translocation and impair AR binding to DNA [19]. In chemotherapy-naïve men with mCRPC, findings from the international, randomized, double-blind, phase 3, PREVAIL trial demonstrated that enzalutamide improved overall survival (OS; 32.4 months vs. 30.2 months; hazard ratio [HR], 0.71; 95% confidence interval [CI], 0.60–0.84; p<0.001) and radiographic progression-free survival (rPFS; not yet reached vs. 3.9 months; HR, 0.19; 95% CI, 0.15–0.23; p<0.001) [20]. PREVAIL data showed that the benefit of enzalutamide extended to all secondary end points, including the time until the first skeletal-related event (SRE), soft-tissue response rate, time until PSA progression, and PSA response rate (≥50% decline), as well as patient-reported outcomes [20212223]. Enzalutamide was approved in Korea in June 2013 for use in men with CRPC postchemotherapy based on results of the AFFIRM trial. In May 2015 the indication was expanded to include men with CRPC regardless of prior chemotherapy exposure based on results of the PREVAIL trial [24].
In this post hoc analysis, we evaluated the treatment effects, safety, and pharmacokinetic exposure of enzalutamide versus placebo in PREVAIL patients from Korean study sites, as well as the consistency of these results with those in the overall population.
MATERIALS AND METHODS
1. Study design and patients
The full methodology of PREVAIL (NCT01212991), including patient eligibility, end point definitions, and study conduct has been reported [20]. PREVAIL was approved by the independent review board at each participating site and was conducted according to provisions of the Declaration of Helsinki and Good Clinical Practice Guidelines of the International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use.
Briefly, consenting patients were chemotherapy-naïve men aged at least 18 years with histologically or cytologically confirmed adenocarcinoma of the prostate that was castration resistant, with evidence of progression by imaging and/or testosterone level of 1.73 nmol/L (50 ng/dL) or less. Eligible patients had not received abiraterone acetate, had an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 (asymptomatic, fully active) or 1 (ambulatory but restricted in strenuous activities), and were asymptomatic or mildly symptomatic based on the Brief Pain Inventory Short Form question 3 (i.e., pain score 0–3) [25]. Medical castration with a gonadotropin-releasing hormone analog was required in patients without orchiectomy. Concomitant use of corticosteroids was permitted with doses equivalent to 10 mg/d of prednisone or prednisolone. Patients with visceral disease or with New York Heart Association class I or II heart failure were eligible. Patients with conditions that could lower the seizure threshold (e.g., brain metastases, history of seizure, concurrent medications), prior use of chemotherapy, or New York Heart Association class III or IV heart failure were excluded.
Patients were enrolled from September 2010 through September 2012 at 207 sites globally, seven of which were in Korea. Korean sites enrolled patients from November 2011 through September 2012. Patients were randomized 1:1 to receive either oral enzalutamide 160 mg (Medivation Inc., San Francisco, CA, USA and Astellas Pharma Inc., Northbrook, IL, USA) or placebo once daily, with randomization stratified by study site. Treatment was discontinued for occurrence of unacceptable side effects, confirmed radiographic progression, or confirmed SRE and either initiation of cytotoxic therapy or an investigational agent for prostate cancer.
2. Assessments
The coprimary end points were rPFS determined by independent central review and OS. Radiographic progression-free survival was defined as the time from randomization to the first objective evidence of radiographic disease progression assessed by a blinded independent central review facility or death due to any cause within 168 days after treatment discontinuation, whichever occurred first. Radiographic disease progression was evaluated using the Prostate Cancer Clinical Trials Working Group [12] guidelines for bone disease and Response Evaluation Criteria In Solid Tumors version 1.1 for soft-tissue disease [26] and included confirmed new bone lesions and new soft-tissue lesions. Imaging was performed at screening, at weeks 9, 17, and 25, and every 12 weeks thereafter. Overall survival was defined as the time from randomization to death from any cause.
Secondary end points included rPFS by investigator review, time to initiation of chemotherapy, time to PSA progression, PSA response, overall soft-tissue response, and time to SRE. Time to initiation of chemotherapy was defined as the time from randomization to initiation of an antineoplastic agent for prostate cancer. Time to PSA progression was defined as the time from randomization to first confirmed PSA progression. PSA response was defined as a decline in PSA of at least 50% from baseline as determined by the local laboratory (confirmed by a second assessment conducted ≥3 weeks later). Time to SRE was defined as the time from randomization to first occurrence of radiation therapy or surgery to bone for prostate cancer, pathological bone fracture, spinal cord compression, or change of antineoplastic therapy to treat bone pain.
Safety was evaluated in all randomized patients who received at least one dose of study drug. Adverse events (AEs) were graded according to the Common Terminology Criteria for Adverse Events version 4.
In all patients, blood was collected for the determination of predose minimum plasma concentrations (Cmin) of enzalutamide and its active metabolite N-desmethyl enzalutamide at weeks 5, 13, and 25. The samples were stored at –70℃ until required for analysis by Covance (Princeton, NJ, USA), as described elsewhere. Briefly, both analytes were extracted from plasma by a liquid-liquid extraction procedure, separated by reversed phase high-performance liquid chromatography, and detected by tandem mass spectrometry, in accordance with U.S. Food and Drug Administration guidance [27]. The quantitation for both analytes was 0.02 to 50.0 µg/mL.
3. Statistical analysis
A post hoc analysis of patients enrolled in Korean study sites at the time of study entry was performed for the coprimary end points, AEs, and all secondary and exploratory end points. Final results for the entire PREVAIL study were based on 439 centrally assessed rPFS events (cutoff date May 6, 2012) and 540 deaths (cutoff date September 16, 2013). Patients randomized after May 6, 2012, were not included in the final rPFS analysis. Thus, an analysis of investigator-assessed rPFS at the final OS data cutoff date (September 16, 2013) and an updated exploratory analysis of OS at the prespecified final number of deaths (≥765; cutoff date June 1, 2014) were also performed.
In this post hoc analysis, baseline characteristics and treatment effects were evaluated in the intent-to-treat population (all randomly assigned patients). Estimates of medians and 95% CIs were determined using the Kaplan-Meier method. The HR relative to placebo, with <1.00 favoring enzalutamide, was determined using an unstratified Cox regression model with treatment as the only covariate.
The mean minimum concentration of the sum of enzalutamide plus N-desmethyl enzalutamide at weeks 5, 13, and 25 were adjusted for weight using log-linear regression. The relative systemic exposure to the sum of enzalutamide plus N-desmethyl enzalutamide in Korean and non-Korean patients was expressed as the ratio of their weight-adjusted Cmin values, including 90% CIs.
RESULTS
1. Patients
The May 6, 2012, cutoff date for the protocol-specified interim analysis of centrally assessed rPFS after 439 events in the overall PREVAIL population occurred during the enrollment period in Korea, thus 38 patients did not have rPFS evaluated by central review (Fig. 1). The investigatorassessed rPFS and OS results, as well as all other metrics, are reported using a data cutoff of September 16, 2013, determined by the occurrence of 540 protocol-specified deaths in the overall study population; at this date all Korean patients had enrolled.
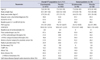
Seventy-eight of 1,717 PREVAIL patients were enrolled at Korean study sites (enzalutamide, n=40; placebo, n=38). Baseline demographic and disease characteristics were well balanced between the enzalutamide- and placebo-treated Korean patients, except that the proportion of patients with an ECOG PS of 0 was lower, and the proportion of patients with bone disease or with a prior radical prostatectomy was higher in the enzalutamide than placebo group (Table 1). Compared with the overall study population, Korean patients had lower median body weight and body mass index, less baseline pain, lower median PSA, less baseline use of corticosteroids, greater use of prior antiandrogens, and greater use of hormonal therapies, and more had a Gleason score of at least 8 at initial diagnosis.
Among Korean patients, median duration of treatment was more than twice as long in the enzalutamide as in the placebo arm (13.0 months vs. 5.1 months). More Korean patients in the enzalutamide group than in the placebo group received at least 12 months of treatment (65% vs. 32%) and continued to receive treatment as of the September 16, 2013, data cutoff date (53% vs. 18%).
2. Treatment effects
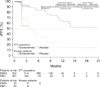
In the final PREVAIL analysis of Korean patients, enzalutamide was associated with a 77% reduction in the risk for centrally assessed radiographic progression or death (HR, 0.23; 95% CI, 0.02–2.24; Fig. 2). In Korean patients, median rPFS by central assessment was not yet reached in the enzalutamide and placebo groups. For rPFS, the treatment effect associated with enzalutamide versus placebo in Korean patients was similar to that observed in the overall study population.
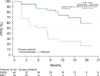
Despite the limited number of patients available for centrally assessed rPFS, a similar relative risk was evident when rPFS was investigator assessed (HR, 0.22; 95% CI, 0.11–0.46; Fig. 3). Median investigator-assessed rPFS was not yet reached in the enzalutamide group (95% CI, 13.6–not yet reached) versus 8.0 months in the placebo group (95% CI, 1.9–8.4).
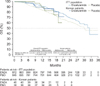
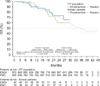
Risk of death was reduced by 23% in Korean patients treated with enzalutamide (HR, 0.77; 95% CI, 0.28–2.15) relative to those who received placebo (Fig. 4). In the updated analysis of OS (June 1, 2014) that included an additional 9 months of follow-up, the risk of death in Korean patients was reduced by 24% (HR, 0.76; 95% CI, 0.34–1.68) with enzalutamide relative to placebo (Fig. 5).
With the exception of median time until first SRE, enzalutamide was associated with improved outcomes versus placebo in Korean patients for all secondary end points (Table 2), as evidenced by longer median times to cytotoxic chemotherapy and PSA progression and better PSA response rates.
3. Subsequent antineoplastic and endocrine therapies
Among Korean patients, subsequent therapies were used by 18% and 66% of enzalutamide- and placebo-treated patients, respectively (Table 3). The most common subsequent therapies received by Korean patients were docetaxel (13% and 58%, respectively) and abiraterone acetate (2.5% and 10.5%, respectively).
4. Safety
The incidence and nature of AEs emergent in Korean patients treated with either enzalutamide or placebo were comparable to those observed in patients treated with enzalutamide or placebo in the overall safety population (Table 4). The median treatment durations for the enzalutamide and placebo groups were 13.0 and 5.1 months, respectively. Among Korean patients, the incidence of AEs of grade 3 or greater was higher in the enzalutamide group than in the placebo group (33% vs. 11%, respectively), although none were considered to be treatment related. The most frequent AEs (with >20% incidence) in enzalutamidetreated Korean patients were fatigue and upper respiratory tract infection, most of which were grade 2 or less. No seizures were observed in Korean patients.
5. Pharmacokinetics
The mean Cmin of the sum of enzalutamide and N-desmethyl enzalutamide in Korean and non-Korean patients at 5, 13, and 25 weeks are presented in Table 5. The Cmin values of enzalutamide plus N-desmethyl enzalutamide at all of these time points were similar in Korean patients and non-Korean patients, with geometric mean ratios (Korean:non-Korean) of 0.97, 1.04, and 1.03, respectively.
DISCUSSION
In this post hoc analysis of asymptomatic or mildly symptomatic Korean men with chemotherapy-naïve mCRPC who participated in the PREVAIL study, treatment effects observed with enzalutamide versus placebo were consistent with those observed in the overall study population, including centrally assessed rPFS (data cutoff May 6, 2012), investigator-assessed rPFS (data cutoff September 16, 2013) and a range of secondary end points.
Some differences in baseline disease characteristics were observed in the Korean subgroup relative to the overall study population, which were likely related to difference in clinical practice. A higher percentage of Korean patients had a Gleason score of at least 8 suggesting a higher disease burden, yet they reported less pain and had a lower median PSA level at baseline. Compared with the overall population of PREVAIL, a larger proportion of Korean patients received prior antiandrogen therapy, which possibly contributed to the lower baseline median PSA level. Unlike the overall study population, no Korean patients received corticosteroids at baseline.
Aside from differences in clinical practice, some differences between the baseline characteristics of Korean patients and the overall PREVAIL population may be related to ethnicity. In men without prostate cancer, several studies have shown that Asian men have a lower baseline PSA than Caucasians [2829]. It is uncertain if this difference in PSA levels between ethnicities signifies that Korean patients have a lower disease burden. Regardless, the difference in the proportion of patients with confirmed PSA responses (i.e., ≥50% reduction from baseline) between the enzalutamide-treated and placebo-treated Korean patients was large (70% vs. 11%), suggesting that regular PSA monitoring may help physicians evaluate treatment response.
As in the overall study population, Korean patients receiving enzalutamide had a more than 2-fold longer duration of therapy than those receiving placebo, and incidences of AEs were similar between Korean patients and the overall study population. Importantly, there were no drug-related AEs of grade 3 or greater in Korean patients and no instances of seizure in Korean patients or the overall study population.
As with other post hoc analyses, limitations apply when interpreting these results. Notably, PREVAIL was not designed to assess differences between enzalutamide and placebo in the Korean subgroup given the small number of Korean patients included in the study, limited follow-up duration, and low number of events. These limitations lead to median estimates of OS and rPFS that could be considered tentative at the time of analysis and a restriction on the ability to detect differences between the AEs of enzalutamide- and placebo-treated patients. Acknowledging these limitations, we sought to examine the consistency of the results in Korean patients with those in the overall study population, which was powered sufficiently to detect the treatment effects and safety of enzalutamide versus placebo.





 XML Download
XML Download