

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Pulmonary artery aneurysm (PAA) is a very rare but can be a fatal disease. If it is not appropriately diagnosed and treated, the patient can develop massive bleeding, ultimately leading to death. PAA can be caused by hereditary factors (persistent ductus arteriosus [PDA], ventricular septal defects [VSD], to others) or acquired infection (syphilis, tuberculosis, to others). PAA has also been reported to be idiopathic, without a specific cause [12]. The symptoms of PAA are diverse and uncharacteristic, ranging from absence of symptoms, dyspnea, chest pain, palpitations, pulmonary embolism, hemoptysis, aneurysmal rupture, to others. Approximately one-third of reported patients died due to PAA rupture, according to a review of the literatures. To diagnose PAA, contrast-enhanced computerized tomography (CT) is primarily used; magnetic resonance imaging (MRI) has also been reported as a diagnostic tool for PAA. It is important to promptly diagnose and treat PAA to reduce the mortality rate, but the optimal therapeutic approach or guidelines remain unclear [12]. The authors of the present study performed an autopsy of a patient who was receiving treatment for tuberculosis and died after bronchoscopic biopsy of a PAA mimicking a bronchial polyp. Case reports on PAA are not rare, but case in which PAA was mistaken for a bronchial polyp and death occurred while performing a biopsy has been seldom reported [34567]. Accordingly, the authors report such a case with autopsy findings.
Case Report
The deceased patient was a 68-year-old woman who underwent a Bentall operation with valve graft one year ago and was taking an anti-coagulant agent following the operation. Approximately 2 months ago, she visited the hospital with a chief complaint of hemoptysis, and was diagnosed with tuberculosis and treated with drug therapy. Bronchoscopy performed at the initiation of therapy revealed a blocked bronchus in the middle lobe of the right lung, due to a nodular lesion. Endobronchial tuberculosis and inflammatory polyp were suspected, but biopsy was not performed due to the risk of bleeding, as the patient was receiving anti-coagulant therapy. Subsequently, the patient was referred to another hospital as an outpatient, in the region in which she resided, and bronchoscopy was planned at a subsequent visit. On the day when bronchoscopy was performed, massive bleeding occurred following biopsy of the area suspected to be a bronchial polyp in the middle lobe of the right lung. Although the patient's posture was changed and bronchoscopic suction was continuously performed, her face and lips became pale and bleeding persisted. In spite of continuous infusion of intravenous fluids, cardiac arrest occurred approximately 30 minutes after the biopsy; cardiopulmonary resuscitation (CPR) was performed, but the patient ultimately died.
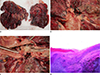
The corpse was stored in a morgue and an autopsy was performed 14 days after death. The deceased was 167 cm tall and weighed 62 kg. Weak postmortem lividity was observed in the back of the body, and the skin of the entire body, the palpebral conjunctivae, and the oral mucosa were pale. External examination showed an old, vertical, surgical scar in the abdominal area, bruising of iatrogenic origin in the abdominal area and the bilateral chest, and other iatrogenic injuries (e.g., needle marks) of the bilateral clavicles, the inguinal area, and in several areas of all limbs. Internal examination showed injuries in the chest area due to CPR and old surgical scars in the abdominal area, heart, and ascending aorta. The right and left lungs weighed 654 g and 460 g, respectively. Pulmonary congestion and a tuberculosis nodule were found in the right lung, as well as a chessboard appearance on sectioning of the right lung (Fig. 1A). Evidence of tuberculosis currently under treatment was observed in the histopathological examination of the middle lobe of the right lung. When pulmonary-bronchial resection was performed, blood was found in the bronchus. The pulmonary artery in the right lobe running parallel with and anterior to the right bronchus formed a round hard PAA in the middle lobe. The PAA protruded into the bronchus, and the end of the protruding PAA was torn (Fig. 1B, C). On histopathological examination, chronic granulomatous inflammation and multinucleated giant cells with necrosis and chronic inflammatory cell infiltration were found in the center of the bronchus and the artery, and calcification of the wall of the protruded PAA was confirmed (Fig. 1D). The PAA was filled with blood clots. On gross examination, the heart showed evidence of prior Bentall operation with valve graft; histopathological examination of the heart showed signs of ischemic heart disease (Fig. 2). Apart from the features reported above, there were no specific findings in other organs.
The deceased patient reported in this case study had visited the hospital due to hemoptysis, was diagnosed with and treated for tuberculosis, developed massive bleeding immediately after undergoing bronchoscopic biopsy of the area suspected to be a bronchial polyp, and finally died. Autopsy and postmortem histopathological examination confirmed a ruptured PAA. According to the patient's medical record, a large massive bleed suddenly occurred and persisted despite bronchoscopic suction, and evidences of hypovolemia and aspiration of blood were observed in the autopsy. Therefore, it was determined that the PAA ruptured while performing the bronchoscopic biopsy and the patient died due to hypovolemic shock and aspiration of blood caused by massive bleeding.
Discussion
PAA is rare and there are few reported cases; thus, its pathophysiology has not been well investigated. It is reported that 89% of all PAA cases occur in the main pulmonary artery and 11% occur in a pulmonary branch artery [8]. The PAA in the present case was located in the main pulmonary artery. Hereditary causes of PAA include heart disease (such as PDA and VSD) and connective tissue abnormality (such as Ehlers-Danlos syndrome and Marfan syndrome), while acquired causes of PAA include infectious disease (such as syphilis and tuberculosis), vasculitis (such as Behcet syndrome), pulmonary artery hypertension, chronic pulmonary embolism, neoplasm (such as lung cancer), and iatrogenic factors (such as heart surgery and catheter placement). Moreover, PAA has been reported to be idiopathic without a specific cause [2]. Among PAA symptoms, hemoptysis is indicative of imminent rupture [2]. The patient in this case study visited the hospital with a chief complaint of hemoptysis and was diagnosed with tuberculosis. A PAA, suspected to be a bronchial polyp, was found during bronchoscopy and ruptured during biopsy of the lesion. Histopathological examination performed on the PAA and surrounding tissue during autopsy confirmed the presence of tuberculosis. Based on the autopsy findings, the cause of PAA in the present case was determined to be tuberculosis.
PAA is rare and it is not easy to confirm at autopsy. If a large quantity of blood is found in the airway and blood is present in the stomach, hemoptysis or hematemesis can be suspected, in which case specific autopsy procedures should be performed to determine the cause of bleeding. To determine the cause of hemoptysis, detailed examination of the bronchus and the lung parenchyma is required, while the entire esophagus including the pharynx and the gastrointestinal tract should be examined to determine the cause of hematemesis. In clinical practice, PAA is diagnosed primarily by contrast-enhanced CT, and postmortem diagnosis of PAA can also be made using postmortem CT angiography [29]. Additionally, histopathological examination may be required to determine the cause of PAA, and in the present case, tuberculosis was confirmed as the underlying etiology.
PAA rupture can be fatal. Particularly if the PAA adheres to a bronchus and protrudes into the bronchus, it can rupture during invasive procedure, such as bronchoscopy; as a consequence, a medical dispute may develop. Choi et al. [5] reported that a bronchial artery aneurysm ruptured during bronchoscopy; however, the patient's status improved after endotracheal intubation and emergency pulmonary resection were performed immediately. The doctor should determine that the mass is an artery by pressing the lesion with forceps to feel pulsation while bronchoscopy is performed; this technique can be used to diagnose a patient in whom the aneurysm protrudes inside a bronchus through the weak bronchial wall due to inflammation, in order to prevent a fatal complication such as PAA rupture [5]. If a biopsy is performed on the basis of an incorrect suspicion of polyp, as in the present case, the doctor should check for pulsatile arterial bleeding after biopsy. If a ruptured aneurysm is suspected, endotracheal intubation must be performed immediately, and surgical resection must be undertaken as soon as possible [5]. An autopsy revealed that the ruptured lesion in this case was not a bronchial but a PAA and that the wall of the PAA was calcified. Accordingly, it is speculated that the PAA ruptured following the biopsy, leading to sudden massive bleeding, and that it would have been difficult to examine pulsation during bronchoscopy due to calcification of the PAA wall. Therefore, if in practice, a patient with a causative disease of PAA has a nodular lesion in a bronchus, additional medical tests such as pulmonary arteriography or chest CT should be performed to examine for the presence or absence of PAA.
Cases have been reported outside of Korea in which bronchoscopic biopsy was performed on a PAA mimicking a bronchial polyp, but in Korea, an autopsy report of such a case has not been published [7]. Thus, the authors of this article report the present case to provide information on this rare entity.

 XML Download
XML Download