

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Desmoid tumors are rare tumors and are characterized by aggressive fibroblastic proliferation (1). The risk of developing a desmoid tumor increases more than 800-fold in patients with familial adenomatous polyposis including Gardner syndrome (1). Desmoid tumors are non-malignant and do not metastasize, but they can be fatal through local invasion (1). This tumor has infiltrative features and can result in urinary tract obstruction, and occasionally, an abscess or fistula (1). However, ureteral fistulas caused by desmoid tumors are rarely reported (234).
Renal scintigraphy using Tc-99m diethylenetriamine pentaacetic acid (DTPA) has been widely used to evaluate renal function and true obstructive uropathy. Furthermore, some studies have reported the utility of renal DTPA scintigraphy for detecting abnormal formation of the urinary tract (35).
We report a case of a patient with Gardner syndrome, in whom renal scintigraphy with Tc-99m DTPA revealed bilateral ureterotumoral fistulas caused by an intra-abdominal desmoid tumor, which changed the treatment plan.
CASE REPORT
A 35-year-old woman with Gardner syndrome presented to our medical center with abrupt onset abdominal pain. She had undergone total colectomy at the age of 29 years, and a mass lesion in the small bowel mesentery detected 1 year previously was histologically confirmed to be a desmoid tumor (Fig. 1). She was subsequently treated with several chemotherapy cycles for the desmoid tumor, but the tumor did not respond. She had undergone a right percutaneous nephrostomy (PCN) during chemotherapy due to hydronephrosis caused by the desmoid tumor. The patient's vital signs were stable on admission. Laboratory results revealed the upper normal limit of the white blood cell (WBC) count (10.2 × 103/µL; normal range, 4.0–10.8 × 103/µL), a low hemoglobin level (9.7 g/dL; normal range, 12.0–16.0 g/dL), a low platelet count (100.0 × 103/µL; normal range, 130–400 × 103/µL), a normal creatinine level (1.2 mg/dL; normal range, 0.5–1.2 mg/dL), and a high C-reactive protein level (69.8 mg/dL). The results of a WBC differential test revealed a high differential neutrophil count of 92.2%.
Contrast-enhanced abdominal computed tomography (CT) was performed to evaluate the abdominal pain, which revealed the already identified desmoid tumor in the small bowel mesentery but no significant interval change in its size compared to that on the previous CT scan. However, a new 5 cm in size poorly-enhanced infiltrative mass lesion containing fluid and a small air density was detected at the mesenteric root (Fig. 1). An abscess combined with the desmoid tumor was suspected. Percutaneous drainage (PCD) of the new cystic mass lesion was performed. After PCD and antibiotic treatment, the cystic mass lesion shrank, but it continued to drain. The color of the leaking fluid was clear and yellowish, suggesting urine. No definite connection was observed between the ureter and the new mass lesion on CT, but a right ureterotumoral fistula was suspected based on the location of the mass. We suspected a right ureterotumoral fistula and an urinoma from urine leakage based on the CT findings and planned to surgically resect the mass and urinoma and repair the right ureter.
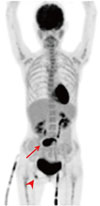
Tc-99m DTPA renal scintigraphy was performed preoperatively to assess the ureterotumoral fistula. Cut-off of the radioactivity was observed at bilateral mid-ureters during the excretion phase on dynamic renal scintigraphy images, suggesting bilateral ureterotumoral fistulas (Fig. 2). No radioactivity was observed in the cystic mass lesion because of PCD. On the other hand, radioactivity was found in the urine contained in the PCD tubes and the PCN tubes and urinary bladder, confirming the presence of an ureterotumoral fistula. F-18 fluorodeoxyglucose (FDG) positron emission tomography (PET)/CT was also performed to detect a hidden malignancy other than the desmoid tumor (Fig. 3). The PCD tube was locked just before the PET/CT scan and urine activity was seen instantly inside the cystic mass lesion. No abnormal increase in FDG uptake was detected to suggest a hidden malignancy, and the desmoid tumor lesion only showed a mildly increased FDG uptake.
As unexpected bilateral ureterotumoral fistulas were detected on renal scintigraphy, removal of the tumor could result in bilateral ureteral dysfunction. Therefore, the treatment plan was changed from surgical resection to conservative management with medication. The patient has been receiving regular clinical follow-up at our medical center.
DISCUSSION
Renal scintigraphy is a very sensitive and non-invasive modality for evaluating renal function and detecting urinary leakage (10). Our patient was clinically suspected to have an ureterotumoral fistula due to the desmoid tumor; however, contrast-enhanced CT images did not reveal a definite connection between the ureter and the mesenteric mass lesion. As functional nuclear images can detect pathological lesions early before significant anatomical changes, we were able to diagnose the involvement of bilateral ureters by the tumor and change the treatment plan. However, although renal scintigraphy demonstrated bilateral ureterotumoral fistulas, the anatomical location of the fistulas was not clear. Renal scintigraphy using a gamma camera integrated with CT would be more helpful in this case. Hybrid single photon emission computed tomography/CT imaging provides both functional and anatomical information, which demonstrates the superior diagnostic value of functional-anatomical hybrid imaging (56).
The optimal treatment for desmoid tumors is controversial and difficult to determine. Clinical follow-up with close observation is recommended for stable asymptomatic patients with a desmoid tumor (1). However, surgical removal is considered to be the first-line treatment for symptomatic patients, and complete resection of the desmoid tumor with negative microscopic resection margins is the standard goal (1). However, many clinicians are reluctant to perform a surgical resection because of the high recurrence rate. Moreover, the surgical trauma could cause a recurrence by itself (789). Complete surgical resection of an intra-abdominal desmoid tumor is extremely difficult and it may be impossible in some cases (17). Because incomplete surgical removal produces a high risk of recurrence and a second operation for treating a recurrent tumor is very difficult to perform due to the intra-abdominal adhesions caused by the previous operation, the surgical approach for an intra-abdominal desmoid tumor should be considered cautiously (2). In addition, patients with familial adenomatous polyposis-associated desmoid tumors have an even higher risk of recurrence (1). Our patient was diagnosed with Gardner syndrome and had had a refractory desmoid tumor with right hydronephrosis. Because of the new symptoms and urine leakage, complete surgical removal of the desmoid tumor and urinoma with repair of the right ureter was preferentially considered, in spite of the deteriorated right ureter function. However, because Tc-99m DTPA renal scintigraphy demonstrated bilateral ureterotumoral fistulas, conservative management was selected to avoid complications that may occur after surgical resection.
We report a case of a patient with an intra-abdominal desmoid tumor who showed unexpected bilateral ureterotumoral fistulas on Tc-99m DTPA renal scintigraphy. Tc-99m DTPA renal scintigraphy was helpful to confirm the diagnosis of an ureterotumoral fistula and to decide the treatment plan.


 XML Download
XML Download