

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Neurolymphoma (NL) is rare neurologic manifestation of hematologic malignancy and involves by infiltration of neoplastic lymphocytes in non-Hodgkin's lymphoma (NHL) or leukemia (123). Its accurate frequency is not known, but it is estimated to occur in 0.2% of NHL cases (4).
NL of the central nervous system is well documented and relatively common, but NL involving the peripheral nervous system occurs even more rarely. Most NLs involving the peripheral nervous system occur secondary to hematogenous spread from systemic NHL or direct infiltration from adjacent structures (5). In contrast, primary lymphoma arising from the peripheral nervous system is quite rare and detailed radiologic information is not readily available since the few previous reports are limited to clinical descriptions (6). We report a case of primary NL mainly involving the tibial nerve and describe its imaging features on magnetic resonance imaging (MRI) and differential points with those of malignant peripheral nerve sheath tumor. This report was approved by our Institutional Review Board.
CASE REPORT
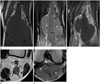
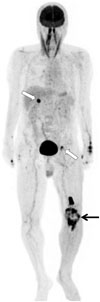
A 77-year-old male patient complained of pain in the left popliteal area after sitting for a couple of hours. A past medical history and systematic review were unremarkable. On physical examination, he had mild numbness along the left lower leg. Plain radiography showed a bulging contour with increased soft tissue density at the posterior aspect of the left knee without bony abnormality. On MR examination, he had a lobulated globular mass measuring approximately 7.2 × 6.7 × 2.0 cm in the popliteal fossa between the gastrocnemius medial and lateral heads (Fig. 1). The mass was fusiform shape by diffuse thickening along the tibial nerve tapering up and down. It also extended superiorly to the distal portion of the sciatic nerve and involved the proximal portion of the common peroneal nerve. In total, the lesion had two components: a globular portion and a fusiform portion. The globular portion appeared as a mass enveloping the thickened continuous nerve bundle. The entire length of the above lesion along the nerve bundle was approximately 18 cm. On both T1-weighted [repetition time (TR)/echo time (TE), 758/13] and T2-weighted (TR/TE, 4043/105) axial images, the lesion was of intermediate signal intensity with multiple dark signal foci within the mass. The dark signal foci revealed two patterns. In the globular portion, the dark signal foci were irregular and relatively short. In contrast, in the fusiform portion as well as the center of the globular portion, which continued to the fusiform portion, the dark signal foci were fine and dot-like on axial images and linear or striated on coronal and sagittal images, suggestive of displaced nerve fascicles by interspersed tumor infiltration. After injection with gadolinium, subtle peripheral enhancement of the mass was demonstrated. The adjacent popliteal artery and vein were totally encased by the mass at the knee joint level, and there was no deep vein thrombosis. The surrounding fat layer and proximal calf muscles showed mild edematous change. 18F-fluorodeoxyglucose (FDG)-positron emission tomography was performed to evaluate the metabolic activity of the lesion and the presence of metastases (Fig. 2). The lesion showed marked FDG uptake [maximum standardized uptake value (maxSUV) 15.8] at the peripheral enhancing portion of the mass and the expected path of the tibial nerve. In addition, small left external iliac and porta hepatis lymph nodes showed FDG activity (maxSUV 6.1 and 8.6, respectively) compatible with metastases.
An approximately 2.0 × 2.0 × 1.0 cm aggregating specimen was obtained from surgical biopsy of the main mass. Microscopic examination revealed diffuse proliferation of atypical lymphoid cells with irregular nuclear folding and occasional prominent nucleoli and pleomorphic nuclei. Immunohistochemical staining showed BCL-6 (+), BCL-2 (+), CD10 (-), CD20 (+), and CD3 (-). The final diagnosis was high grade B-cell lymphoma (diffuse large B-cell lymphoma). The patient was referred to the department of oncology and treated with a chemotherapy protocol [rituximab, cytoxan, hydroxydaunorubicin, oncovin, and predinisolone (R-CHOP)] with radiotherapy. After 2 months of treatment, the main mass and metastatic lymph nodes decreased in size and activity.
DISCUSSION
NL of the peripheral nerve is a rare disease; its precise incidence is not well known. NL usually occurs as secondary or systemic involvement related to previously known hematologic malignancies such as lymphoma or leukemia (1). It is almost always related to NHL and the most common type of lymphoma is diffuse large B-cell lymphoma, followed by follicular lymphoma. Although the involvement of peripheral nerves as disseminated systemic lymphoma or direct extension from contiguous lymphoma has been previously described, primary lymphomas of the peripheral nerve are quite rare (67). The most frequently involved site of primary lymphoma of the peripheral nerve is the sciatic nerve, but it is unclear why there is a predilection for the sciatic nerve (8). Quiñones-Hinojosa et al. (9) postulated that B-cells may stay or originate in the sciatic nerve and a specific cell adhesion molecule expansion may be the basis for tissue targeting, but these molecules have not been identified. In addition, those a few cases were reported in the brachial plexus, ulnar, median, and radial nerves and the sympathetic chain (8). Our case was the first report of a primary NL originating from the tibial nerve and its MRI findings.
Clinical diagnosis with physical examination can be difficult because NL can mimic many other conditions and its presenting symptoms are diverse depending on the sites involved. Such symptoms include painful or painless mononeuropathy, painful radioculopathy, cranial neuropathy, and polyneuropathy (123); there are also cases without symptoms. Our patient had only mild numbness and pain of involved area after being in the sitting position for a long period of time. Given the unclear clinical manifestations and rare incidence of NL, radiologic evaluation and histologic examination are required for appropriate diagnosis and proper management. Radiological evaluation using MRI can be helpful for differential diagnosis from other masses and assessment of the extent of the lesion, though surgical biopsy of the involved structure is the gold standard (3). Appropriate diagnosis of NL and early management will prevent complications and perhaps morbidity (2).
Imaging features of NL include diffuse enlargement of the peripheral nerve and mass formation along the course of the involved nerve with or without contrast enhancement (12). Wadhwa et al. (1) reported NL often shows areas of interspersed minimal heterogenous hypointensity (dark spots) within the mass on T2WI, although the cause of these findings is unclear. Our case also showed fine dot-like dark signal foci on axial image and these showed linear structures that continued to the nerve fascicles along the fusiform portion of the lesion on coronal and sagittal images. We can speculate that these findings may be related to the characteristics of lymphoma, which tend to preserve the shape or contour of the involved structure or encase the adjacent structures rather than invade or destroy the tissue. In the same way, the findings of the popliteal artery and vein that was encased in the mass can also help characterize the lymphoma. On MRI, therefore, diffuse enlargement of the peripheral nerve and mass formation with findings suggesting relatively preserved nerve fascicles and vascular structures are important to distinguish lymphoma from other diseases such as malignant peripheral nerve sheath tumors, which usually show characteristic destruction of the nerve architecture within the lesion and heterogeneous features due to their complex components (10).
There is still debate regarding the standard treatment regimen for NL. Generally, systemic chemotherapy alone or a combination of chemotherapy with intrathecal chemotherapy or radiotherapy is performed (34). Our patient was treated with R-CHOP with radiotherapy after surgical biopsy, and the metastatic nodes as well as the mass showed positive therapeutic response after 2 months. The general prognosis of patients with NL is poor in spite of treatment, which may be caused by the lack of a standard regimen (3). Thus, large randomized clinical trials will be needed to establish a standard treatment regimen, and appropriate diagnosis using MRI will contribute to long-term outcomes.
In conclusion, we report the first case of NL involving tibial nerve in association with characteristic MRI findings including homogeneous internal contents for tumor size and preservation of adjacent structures such as interspersed nerve fascicle, which might be useful to differentiate NL from other neurogenic tumors of malignant peripheral nerve sheath tumor.
 XML Download
XML Download