

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Recently, reducing radiation dose to all body parts of children and adults has been a paramount issue in diagnostic radiology (1). Among various techniques used to reduce radiation dose, lowering peak tube voltage has been a clear trend because radiation dose changes approximately with the square of tube potential (2345). Lowering peak tube voltage provides improved contrast enhancement of iodine-containing vascular and parenchymal organs because it provides a greater photoelectric effect with decreased Compton scattering (67). Inevitably, lowering peak tube voltage can lead to greater image noise and poor image quality, thus resulting in decreased diagnostic accuracy. This prevented clinical implementation of techniques for lowering peak tube voltage in the past, particularly in abdominal CT application (8). However, a new algorithm for concurrently adjusting the high-output tube current known as automatic tube current modulation (ATCM) can counterbalance greater image noise at low tube voltages (9). With the advances in ATCM, recent CT scanner can automatically select tube voltage depending on the patients' attenuation profile from CT topogram, thus enabling us to lower tube voltage from 120 kVp to 100 kVp or even 80 kVp (10).
100 kVp chest, pulmonary, or head CT angiographies has been proven to be useful for diagnostic purposes (11121314). Although 100 kVp abdominal CT was effective in older children in a phantom study, a few in vivo studies of lowering the tube potential from the standard 120 kVp to 100 kVp or even 80 kVp for abdominal CT and liver dynamic CT have been reported (151617). However, these studies mainly evaluated hypervascular hepatic lesions, vascular structures, or iodine-filled structures rather than general image quality. In addition, a few in vivo studies of using 100 kVp abdominal CT in adults have been performed with a small number of patients (171819). Therefore, the purpose of this study was to compare image quality of abdominal organs and the effect of radiation dose reduction after decreasing tube voltage from 120 kVp to 100 kVp in abdominal CT in adult patients.
MATERIALS AND METHODS
This study was approved by Institutional Review Board. The requirement of written informed consent was waived since the scan protocol introduced herein was routinely used in all patients undergoing clinically indicated CT at our institution. A total of 200 patients with body mass index (BMI, kg/m2) of less than 30 kg/m2 were enrolled. We excluded obese patients (BMI ≥ 30 kg/m2) because image quality in these patients was empirically poor at a tube voltage of 100 kVp. The abdomen-pelvic CT protocol was consisted of a non-enhanced and a contrast-enhanced series. All patients were scanned from the basal lung to pubic symphysis. We included patients who received only one type of intravenous nonionic contrast medium. In each patient, 100–120 mL of iomeprol (Iomerol®; Bracco, Italy) was injected at a flow rate of 2.5 mL/s without additional saline injection for contrast enhanced series. No oral contrast medium was ingested for gastrointestinal tract opacification. Portal venous phase contrast-enhanced series was obtained at 70–90 seconds after the initiation of contrast material injection. All patients were examined with the same 128-slice MDCT scanner (Somatom Definition Flash; Siemens Healthcare, Forchheim, Germany) from 1st January 2014 to 31st March 2014. One hundred patients (mean age, 64.3 ± 17.2 years; range, 18–89 years, 66 males, 34 female patients) underwent CT with fixed tube potential at 120 kVp (120 kVp group). The other one hundred patients (mean age, 63.8 ± 16.1 years; range 17–90 years, 52 males, 48 female patients) underwent CT with fixed tube potential at 100 kVp (100 kVp group). The algorithm takes into account that the maximum tube current at the prefixed tube voltage can maintain adequate image quality level. The image quality level of attenuation-based tube current modulation (CAREdose 4D; Siemens Healthcare, Forchheim, Germany) corresponded to 289 ref. mAs at 100 kVp and 210 ref. mAs at 120 kVp, respectively. These reference tube current settings were default settings from the vendor. Other CT parameters were kept constant: detector collimation 128 × 0.6 mm; slice collimation 64 × 0.6 mm by means of a z-flying focal spot; pitch, 0.9; and rotation time, 0.5 s. Abdominal CT images were reconstructed using a medium-smooth soft tissue convolution kernel (B40f) without using iterative reconstruction (IR).
Measurement of Radiation Dose
Each patient's effective mAs, volume of the computed tomography dose index (CTDIvol), and dose length product (DLP) provided by the CT scanner were recorded. Estimated effective radiation doses were calculated by multiplying total DLP with the conversion coefficient factor (k = 0.015 mSvmG-1cm-1) (20).
Quantitative Image Quality Analysis
Quantitative assessment of image quality was performed on a PACS work station (Piview, INFINITT Healthcare, Seoul, Korea). One independent and blinded radiologist calculated the mean Hounsfield unit (HU) value for two regions of interest in the liver, pancreas, renal cortex, abdominal aorta above and below the renal artery take off level, main portal vein, and psoas muscle at L4 level. Standard deviation of air outside the patient (HU) was considered as background image noise. Signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) of each organ were calculated using the following equations:


Qualitative Image Quality Analysis
Overall image quality and artifacts were independently and blindly evaluated by two board-certified radiologists with more than 7 years of experience in abdominal radiology. Noise texture, artifacts, and diagnostic acceptability were evaluated using a 4-point scale based on a modified European Quality Criteria scoring system (21). Noise texture were rated with a 4-point scale for the liver, pancreas, renal cortex, and psoas muscles (0, changes affecting serious misdiagnosis or blotchiness; 1, changes probably affecting diagnosis; 2, mild change do not affect diagnosis; 3, average or no change). Artifact and diagnostic acceptability was rated after fully reviewing each CT scan. Artifact was rated with a 4-point scale (0, severe artifact, degraded or affecting diagnosis; 1, moderate artifact affecting the visualization of normal structures; 2, mild artifact not affecting the visualization of any structure; 3, no artifact). Diagnostic acceptability was assessed with a 4-point scale based on the confidence of the radiologist who assessed abdominal findings (0, unacceptable; 1, acceptable under limited condition; 2, probably acceptable; 3, fully acceptable for diagnostic interpretation).
Statistical Analysis
Continuous variables were expressed as means and standard deviations. Interobserver agreement was assessed with weighted kappa (k) statistic (k > 0.81: excellent agreement; k = 0.61–0.80: good agreement; k = 0.41–0.60: moderate agreement; k = 0.21–0.40: fair agreement; k < 0.20: poor agreement). Patient's age, BMI, radiation dose, and quantitative image parameters (attenuation values, image noise, SNR, and CNR), corrected by Welch's test depending on normality testing were tested with independent t-test. Qualitative analysis of image quality was compared using Wilcoxon signed-rank test. Statistical analysis was performed with MedCalc software (MedCalc 13.1.2, Ostend, Belgium). A p < 0.05 was considered as statistically significant.
RESULTS
Demographics and Radiation Dose Analysis
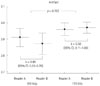
There was no significant (p > 0.05) difference in patient age (64.3 ± 17.2 years vs. 63.8 ± 16.1 years), scan length (54.2 ± 4.6 cm vs. 54.5 ± 6.7 cm), or BMI (23.0 ± 2.9 vs. 23.0 ± 3.6) between the 120 kVp group and the 100 kVp group (Fig. 1). Radiation doses for both protocols are summarized in Table 1. CTDIvol, DLP, and mean effective mAs values in the 120 kVp group and the 100 kVp group were 9.4 ± 3.1 mGy and 8.2 ± 2.2 mGy, 516.2 ± 189.6 and 450.1 ± 148.3, and 139.2 ± 45.8 and 194.9 ± 56.6, respectively (p = 0.0010, 0.0010, 0.0064). A radiation dose reduction of approximately 13.3% was found in the 100 kVp group compared to that in the 120 kVp group.
Quantitative Image Quality Analysis
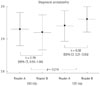
Background image noise (standard deviation of outside air CT number) in the 100 kVp group (10.6 ± 3.8) was significantly (p < 0.0001) higher than that (7.2 ± 1.5) in the 120 kVp group (Fig. 2). CT numbers, SNR, and CNR of each abdominal organ are summarized in Table 2. SNR of all abdominal organs except portal vein in the 120 kVp group was significantly (p < 0.05) higher than that in the 100 kVp group. However, CNR of all abdominal organs except the liver showed no significant (p > 0.05) difference between the two groups. CNR of the liver in the 120 kVp group (8.1 ± 3.8) was significantly (p < 0.05) higher than that (6.7 ± 3.7) in the 100 kVp group. CNR of the aorta and portal vein showed no significant (p = 0.17 and 0.63, respectively) difference between the two groups.
Qualitative Image Quality Analysis
Hepatic noise texture was scored at 2.56 ± 0.50 and 2.60 ± 0.49 on the 100 kVp scan by two readers compared to 2.73 ± 0.45 and 2.80 ± 0.40 on the 120 kVp scan (Fig. 3A). Pancreatic noise texture was scored at 2.80 ± 0.40 and 2.83 ± 0.38 on the 100 kVp scan compared to 2.90 ± 0.30 and 2.85 ± 0.36 on the 120 kVp scan (Fig. 3B). Renal cortex noise texture was scored at 2.85 ± 0.36 and 2.84 ± 0.37 on 100 kVp scan compared to 2.86 ± 0.35 and 2.79 ± 0.41 on 120 kVp scan (Fig. 3C). Psoas muscle noise texture was scored at 2.84 ± 0.37 and 2.91 ± 0.29 on 100 kVp scan compared to 2.85 ± 0.36 and 2.91 ± 0.29 on 120 kVp scan (Fig. 3D). Only hepatic noise texture was significantly (p = 0.0001) different between the two groups. Other noise texture of pancreas, renal cortex, and psoas muscle were insignificant (p > 0.05) between the 100 kVp and 120 kVp scans.
The mean and standard deviation of artifact was scored at 2.91 ± 0.29 and 2.87 ± 0.34 on 100 kVp scan by two readers. It was scored at 2.96 ± 0.20 and 2.97 ± 0.17 by the two readers on 120 kVp scan (Fig. 4). The mean and standard deviation of diagnostic acceptability was rated at 2.93 ± 0.26 and 2.92 ± 0.27 on 100 kVp scan by the two readers compared to 2.94 ± 0.24 and 2.96 ± 0.20 on 120 kVp scan (Fig. 5). The readers had full confidence in 92.5% of the 100 kVp scans and 95% of the 120 kVp scans. There was no significant (p > 0.05) difference in artifact or diagnostic acceptability of both scan protocols according to each reader. Representative case of qualitative analysis is shown in Fig. 6.
DISCUSSION
Automated tube voltage selection and current modulation is an automated attenuation-based, kilovoltage selection software algorithm that simultaneously optimizes the tube potential and tube current selection for each patient. This calculation is based on the patient's attenuation profile measured from CT topogram and the diagnostic task to be performed so that desired image quality and low radiation dose can be achieved. Tube voltage settings include 80, 100, 120, and 140 kVp. Tube voltage matches CNR, a parameter for image quality optimization, at each tube voltage relative to that of a user-defined image quality reference (9).
With this advanced technique, a clear trend towards the use of lower tube voltage CT scans for the brain, heart, chest, and body has been observed in recent years (11121314). In accordance with reduced streaming radiation dose, a low tube voltage of 100 kVp is routinely selected for abdominal CT application of recent state-of-the-art multidetector row CT scanners (10182223). The primary objective of this study was to assess the image quality of portal phase abdominal CT of abdominal organs by lowering tube voltage from 120 kVp to 100 kVp.
Our results indicated that the 100 kVp abdominal CT protocol significantly reduced radiation dose compared to the 120 kVp standard protocol. In this study, the mean CTDIvol at 100 kVp was 8.2 mGy and the mean CTDIvol at 120 kVp was 9.4 mGy. A radiation dose reduction of 13.3% was found with the 100 kVp abdominal CT protocol. This finding was similar to the results of previous reports (16181924). However, the radiation dose used in this study was the lowest among recently published articles.
The mean CT number of each organ and background image noise were higher at 100 kVp, in agreement with reports of other studies (101119). According to the SNR equation, SNR is inversely related to background noise. Thus, low SNR of each organ in the 100 kVp group compared to the 120 kVp group was due to increase in background noise. As the CT number of the psoas muscle became higher with the 100 kVp protocol, it might have caused low CNR of the liver with the 100 kVp protocol than that of the 120 kVp protocol. Even though SNR and CNR between both scan protocols showed significant differences in quantitative analysis, the difference value was equal or less than 4. Such minimal differences are probably not discernible by visual inspection. Therefore, it is difficult to know whether CNR and SNR obtained with the 100 kVp protocol have great effect on diagnosis.
Low tube voltage CT not only can increase image contrast because low-energy X-rays are more strongly attenuated by iodine than by surrounding tissues, but also can increase image noise because low-energy X-rays are captured or absorbed more in the soft tissue, thus decreasing photons that reach the detectors. Greater image noise in low tube voltage CT angiography does not necessarily result in diminished subjective image quality as shown in various clinical investigations because improved iodinated contrast enhancement at lower kilovoltage enable a higher noise to be tolerated while achieving a great radiation dose reduction (1214252627). However, in portal phase abdominal CT, iodine concentration is lower than that in CT angiography. Because detection and characterization of parenchymal lesions require lower noise levels, this necessitates the use of higher tube voltage and radiation dose (8). The disadvantage of lower tube voltage can be compensated by using concurrent high-output tube current (2829). In our study, although the tube current was concurrently increased from 210 mAs to 289 mAs by using the ATCM technique, it was suboptimal to nullify image noise, resulting in an increase in image noise of up to 47% compared to that in other stuides. On qualitative image quality analysis, diagnostic acceptability showed no statistically significant difference between the two groups. However, noise texture of the liver was frequently scored 2 points more by both readers. To reduce image noise, IR could be a tenable option. IR is not applied during abdominal CT application in daily clinical practice at our institution because of concerns of its graphic and pixelated effects. Husarik et al. (16) have demonstrated an approximately 35% of image noise reduction with the 100 kVp protocol in a phantom study using IR compared to the 120 kVp protocol. In addition, Kalra et al. (30) have demonstrated that attenuation by various tissues is not changed when using IR. However, Baker et al. (31) reported that lower dose acquisitions with any reconstructed algorithm had limitation in eva-luating the conspicuity of lesions depending on radiation dose level that low-contrast lesions could not be detected with adequate accuracy. SNR and CNR of abdominal organs were similar between both scan protocols because the difference of SNR and CNR was very small (equal or less than 4). In addition, there was no significant difference in diagnostic acceptability. However, these results do not guarantee similar accuracy in detecting low-contrast lesions such as small hepatic cysts or metastasis. Therefore, further investigation is needed to determine whether low tube voltage abdominal CT with or without IR will accurately detect these low-contrast lesions in abdominal organs.
Our study has some inherent limitations. First, the patient population was heterogeneous with various patient sizes. Radiation dose closely depends on patient size (1532). We excluded obese patients with BMI equal or more than 30 kg/m2. The two protocol groups showed no difference in BMI distribution. However, some minor factors such as uneven distribution of high and low BMI patients or difference in patient's anteroposterior and transverse diameters were not evaluated. Second, we did not evaluate the accuracy of the 100 kVp scan protocol in detecting focal lesions. The SNR and CNR of each target organ showed similar values using both protocols. Therefore, detection of hypervascular lesions should not be an issue. However, as mentioned above, detection of low-contrast lesions may be affected using the 100 kVp scan protocol.
In conclusion, abdominal CT with a low tube voltage of 100 kVp reduced radiation dose by 13.3% without significantly sacrificing image quality. However, low-contrast hepatic lesions such as small cysts or hypovascular metastases should be evaluated more carefully because of the inherent limitations of low tube voltage CT.






 XML Download
XML Download