

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Wilms' tumor is the most common renal neoplasm in children. This tumor typically originates from the renal parenchyma and extents into the surrounding tissues. Rarely, it arises from the renal pelvicalyceal wall, occupying the collecting system with minimal parenchymal involvement which is similar in appearance to that of botryoid sarcoma, resulting in a so-called botryoid Wilms' tumor (12). Botryoid Wilms' tumor is markedly rare, and to the best of our knowledge, only few cases have been reported in the literature with limited imaging findings. Here, we report a case of botryoid Wilms' tumor filling the renal pelvicalyceal system and mimicking a blood clot in a child presenting with gross hematuria, with a focus on ultrasonography (US) and magnetic resonance imaging (MRI) findings.
CASE REPORT
The Institutional Review Board of our hospital approved this case study and waived the requirement for obtaining informed consent.
A 5-month-old boy was referred to our outpatient clinic for evaluation of gross hematuria. The child had no specific medical or family history. Vital signs and observations from the physical examination were within normal limits. Blood cell count results were within normal limits as follows: white blood cell count 9330/µL, hemoglobin level 11.8 g/dL, hematocrit level 35.1%, and platelet count 529000/µL. Random urinalysis with microscopic examination showed numerous red blood cells and white blood cells per high-power field without bacteriuria or proteinuria.
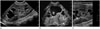
On the clinical impression of urinary tract infection, renal US was performed at our hospital, which revealed multilobulated hyperechoic lesions filling the pelvicalyceal system of the right kidney (Fig. 1). The lesions were compacted in the renal pelvis, causing pelvicalyceal dilatation, and they extended to the proximal ureter. There was no definite renal parenchymal infiltration or invasion. Also, there was fine debris in the dilated calyces and no definite internal vascularity of the lesion on color Doppler study. Even though the lesions did not move during position changes in the patient, the possibility of a compacted blood clot or sludge from infection could not be excluded. We performed follow-up US after one week, which demonstrated the same findings of a lobulated renal pelvic lesion even though antibiotic therapy was initiated. Therefore, MRI with contrast enhancement was performed to evaluate the extent and detailed characteristics of the lesion (Fig. 2). The images of MRI also demonstrated a multilobulated and polypoid lesion in the dilated right renal pelvis and calyces with intermediate to high signal intensity on T1-weighted images and high signal intensity on T2-weighted images. The lesions extended to the right proximal ureter, causing obstructive hydronephrosis of the right kidney with mild renal swelling. There was no definite evidence of hemorrhage or hemosiderin deposit in the lesion. On diffusion weighted images, the lesion demonstrated diffusion restriction. After gadolinium enhancement, the lesion showed delayed heterogeneous enhancement without parenchymal infiltration or invasion. Based on these imaging findings, a diagnosis of renal pelvic tumor with ureteral extension was suggested, and differential diagnoses included Wilms' tumor, mesoblastic nephroma, ossifying renal tumor of infancy, and rhabdoid tumor.
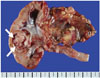
Under generalized anesthesia, retrograde pyelography also demonstrated a multilobulated mass extending from the mid ureter to the dilated renal pelvis of the right renal collecting system. Subsequent laparoscopic radical right nephrectomy was performed. During the operation, there was a jelly-like mass filling the right renal pelvis and lower pole calyx extending to the proximal ureter without renal parenchymal invasion (Fig. 3). The histopathologic examination revealed the triphasic type (blastemal, epithelial, and stromal components) Wilms' tumor arising from the medulla and extending to the calyceal system with botryoid features. The renal sinus, renal capsule, and right ureter were free of tumor, and there was no evidence of cellular anaplasia or lymphovascular invasion. Due to the suspicion of tumor spillage during operation, the patient underwent postoperative chemotherapy with dactinomycin and vincristine combined with radiotherapy targeted to the right flank area. The last follow-up abdominal US and chest computed tomography (CT), which were performed 7 months after the surgery, revealed no evidence of recurrent mass or distant metastasis.
DISCUSSION
Wilms' tumor is the most common malignant renal neoplasm occurring during childhood. The majority of Wilms' tumors arise within the renal parenchyma without evidence of renal pelvic extension. In rare circumstances, intraparenchymal Wilms' tumor extending into the renal collecting system or Wilms' tumor arising within the renal pelvis without intraparenchymal extension is observed. Wilms' tumors with these rare features have a similar pathologic appearance to botryoid sarcoma, and are therefore called botryoid Wilms' tumor (12).
The age of patients diagnosed with botryoid Wilms' tumor ranged from 4 months to 8 years, according to the previous reports (3), including our patient who had been diagnosed at the age of 5 months. The clinical manifestations of botryoid Wilms' tumor are distinct from those of typical Wilms' tumor. An asymptomatic mass is the most common symptom of typical Wilms' tumor, with other symptoms occurring in less than 25% of cases (4). In contrast, in most cases of botryoid Wilms' tumor, the diagnosis was suggested by episodes of gross hematuria or an abdominal mass with or without hydronephrosis (4). The chief complaint of our patient was gross hematuria, and hydronephrosis was detected on US. Since botryoid Wilms' tumor is prone to extend into the proximal ureter, hydronephrosis with or without infection is likely to be an important presenting manifestation (4).
In most patients with suspected abdominal mass or urologic symptoms, US is usually performed initially for the evaluation. There have been several case reports of botryoid Wilms' tumor that provided its sonographic findings such as a renal pelvic mass with mixed echogenicity (24). Occasionally there is an anechoic space inside the mass, probably due to necrosis or hemorrhage (5). There is a rare case report of botryoid Wilms' tumor presenting as bilateral echogenic masses with calcification (6). However, most case reports do not present high resolution images or Doppler imaging findings. The sonographic images provided in our study clearly demonstrate a lobulated and hyperechoic mass filling the pelvicalyceal system without parenchymal invasion, which was also confirmed by pathology. The Doppler study also demonstrated no remarkable vascularity of the mass that could mimic a blood clot. Further studies such as MRI could be performed, as in our case, for the differential diagnosis of the tumor and blood clot.
CT remains the preferred technique for assessment of children with a suspected renal mass. Most case reports of botryoid Wilms' tumor also provide CT findings. The common CT features of botryoid Wilms' tumor are a heterogeneous mass with subtle enhancement (6), almost or completely filling the pelvicalyceal system and extending into the proximal ureter (2457). Occasionally, these tumors extend down the entire course of the distended ureter and protrude into the bladder (26).
Abdominal MRI is often the preferred technique for the evaluation of abdominal masses in young children due to its higher resolution without radiation risk. Moreover, MRI can be superior to CT for the assessment of vascular extension of Wilms' tumor. However, to the best of our knowledge, only one study has reported the MRI features of botryoid Wilms' tumor as an enlarged kidney with a heterogeneous mass occupying a large portion of the collecting system (7). The report did not provide detailed information of the mass such as diffusion restriction or enhancement pattern. The MRI features in our study demonstrated intermediate to slightly high signal intensity on T1-weighted images, diffusion restriction and delayed heterogeneous enhancement. These findings are consistent with typical features of ordinary Wilms' tumor. Even though the renal pelvic lesion in our case mimicked a blood clot on US, these MRI findings suggested a renal pelvic mass.
Other differential diagnosis of renal intrapelvic tumor in an infant can be mesoblastic nephroma, ossifying renal tumor of infancy, rhabdoid tumor, and xanthogranulomatous pyelonephritis (XGP). About 90% of mesoblastic nephromas are discovered before 1 year of age, and they can involve the renal sinus and exhibit benign behavior (8). However, they show infiltrative margins and frequent renal parenchymal involvement. The ossifying renal tumor of infancy is a benign tumor, which typically arises from the urothelium of the renal medulla, and grows into the renal collecting system in a polypoid shape (8). It usually manifests as a filling defect in the collecting system with ossification and poor enhancement (89). Rhabdoid tumor can also be found in an infant; however, this tumor usually presents as an infiltrative centrally located mass with frequent local invasion (9). XGP can present in either a diffuse or focal form. Focal XGP is more common in children and can imitate many neoplastic diseases, especially Wilms' tumor (10). Even though the imaging features are not specific to allow distinction between focal XGP and renal tumors, the accompanying clinical signs of infection or inflammation might suggest the diagnosis of XGP. A lobulated and polypoid mass filling the pelvicalyceal system without parenchymal invasion and absence of inflammatory signs can be unique imaging features of botryoid Wilms' tumor.
In conclusion, despite the rarity of botryoid Wilms' tumor, radiologists should be aware that Wilms' tumor may appear entirely within the renal pelvis or it may extend into the collecting system with minimal or no parenchymal invasion, which can be the typical finding of this tumor in children presenting with hematuria.

 XML Download
XML Download