

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In this article, we reviewed our institutional database and radiology department database of images taken from 2005 to 2013 and retrieved the records of 256 patients who underwent brain CT or MRI and were later diagnosed with tumorous or nontumorous calvarial lesions (122 malignant neoplasms, 115 benign neoplasms, 19 non-neoplastic lesions). The majority of patients either had multiple myelomas (n = 108, 42.2%) or benign osteomas (n = 99, 38.7%) (Table 1). Though calvarial metastases are the most common malignant lesions, multiple myeloma is more common in our database because of errors in coding and also because our institution is renowned for treating hematologic malignancies. We retrospectively reviewed the imaging findings of CT and MRI for these calvarial lesions, and, using a categorical imaging approach, we briefly described and illustrated the imaging findings of representative osteolytic calvarial lesions. The Institutional Review Board approved this retrospective review, and the requirement of informed consent was waived.
CATEGORICAL APPROACH TO IMAGING DIAGNOSIS
With increasing frequency, CT and MRI have been incorporated into the basic imaging tools for evaluating calvarial lesions. Therefore, it is useful to categorize diagnostic features of images taken not by conventional radiography but by CT and MRI (12). It is possible to categorize 8 different types of calvarial lesions based on 4 key features: thickening or thinning of calvarial bone, sclerosis or lysis of bone, focal or generalized lesions, and, finally, singularity or multiplicity of lesions. On CT and MRI, sclerotic lesions appear as thickening of calvarial bone (either the inner/outer tables, or bone marrow, or both). Accordingly, we can simplify the classification system into six categories based on three main features. We suggest that calvarial lesions are classified into calvarial thickening, thinning, and lytic lesion. When the calvarial lesions fall into the 'thickening' or 'thinning' categories, they can be further subdivided into focal or generalized lesions. The lytic category can be subdivided into either single or multiple lesions. Furthermore, we can expect to get additional information about matrix characteristics with contrast enhancement and diverse advanced MR sequences such as diffusion-weighted imaging (DWI) (3), perfusion-weighted imaging, and MR spectroscopy. A flowchart for a systematic approach to imaging diagnosis of calvarial lesions is provided in Table 2.
Single or Multiple Osteolytic Lesions
Multiple Myeloma
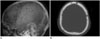
Multiple myeloma is characterized as multiple osteolytic lesions due to the malignant proliferation of osteoclast-activating factors triggered by myeloma. Plain radiography of multiple myeloma patients is characterized by a subcortical circular or elliptical radiolucent shadow, and the axial skeleton is the predominant site of the abnormality. CT shows punched-out lesions with soft tissue masses and fractures. On MRI, multiple myeloma presents with low-to-intermediate signal intensity on T1-weighted images, high signal intensity on T2-weighted images, and high signal intensity on DWI (4). The lesions enhance strongly following contrast administration. Four different imaging patterns may appear: normal-looking marrow, a micro nodular pattern (also described as variegated or salt and pepper lesions), a focal pattern, or a diffuse pattern (Fig. 1) (12).
Osteolytic Metastases
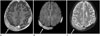
Metastases take various forms; they can be seen as either osteoblastic or osteolytic lesions on plain radiograph. When appearing as single or multiple lytic lesions, metasteses are usually seen as one or more relatively circumscribed intraosseous lesions or sometimes as diffusely destructive on bone algorithm CT (2). Hypointense infiltrating foci are seen on T1-weighted images as metastases replace hyperintense normal yellow marrow. Most skull metastases are hyperintense compared to bone marrow on T2-weighted images and appear clearly on fat-saturated contrast-enhanced T1-weighted images (Fig. 2). DWI is helpful for the detection of bone marrow involvement of the calvarium (3).
Langerhans Cell Histiocytosis
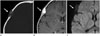
Langerhans cell histiocytosis (LCH) is an uncontrolled monoclonal proliferation of abnormal Langerhans cells involving any organ. When LCH involves the skull, it manifests as a small soft tissue calvarial mass with lytic defect and beveled edge more on the inner table than the outer table on plain radiograph and CT scans. It is often seen as bilateral soft tissue masses with bone destruction. On MRI, LCH presents as an enhancing soft tissue mass on contrast-enhanced T1-weighted images with vivid enhancement of the pituitary infundibulum and stalk thickening (Fig. 3) (567).
Osseous Hemangioma
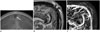
Osseous hemangiomas are benign skull lesions composed of predominantly vascular entities. On plain radiographs and CT scans, they present as sharply defined expansile lesions, which may include a periosteal reaction and be surrounded by a thin peripheral sclerotic rim, as is the case approximately 30% of the time. They show intact inner and outer tables; the outer table tends to be more expanded than the inner table. Trabecular thickening with radiating spicules is also commonly seen. MRI signal strength depends on the quantity of slow-moving venous blood, the proportion of red to fatty marrow, and hypointense trabeculae (8). Osseous hemangiomas are typically hyperintense on T1-weighted images and heterogeneously hyperintense on T2-weighted images. They enhance intensely, heterogeneously, or minimally on contrast-enhanced CT or MRI (Fig. 4) (89).
Epidermoid and Dermoid Cysts
Epidermoid and dermoid cysts are ectodermal inclusion cysts lined by epithelium. They occur inside the orbit, in the calvarial diploic space, and intracranially (9). They typically appear as encapsulated unilocular cystic lesions with a signal intensity that depends on their components (1). On plain radiograph and CT scans, epidermoids appear as intradiploic, expansile, osteolytic lesions with smooth sclerotic margins while dermoids appear as expansile, osteolytic midline lesions. On CT, dermoids contain a soft-tissue component extending to overlying skin and intracranial areas. Usually epidermoids have a fluid-like signal intensity on MRI. Dermoids have a heterogeneous appearance with varied signal intensities depending on their various compositions. Since dermoids contain fatty tissue, they show low attenuation on CT and high signal intensity on T1-weighted images (Fig. 5) (169). Enhancement is generally absent although mild peripheral enhancement can be seen in about 25% of cases.
Intraosseous Meningioma
When a meningioma invades overlying bone, it can create an osteolytic bone lesion. Infrequently, meningioma arises initially in the calvarium. It is thought that trapping of ectopic meningocyte or arachnoid cap cells in the cranial sutures may cause primary intraosseous meningiomas (10). Approximately 68% of primary extradural meningiomas involve the calvarium (11). Primary extradural meningiomas typically present with slow scalp swelling and do not show any neurologic symptoms or signs, unless the lesion extends through the inner table and compresses intracranial structures (12). On plain radiograph and CT, well-defined radiolucent, osteolytic lesions can be seen. On MRI, meningiomas are usually hypo- to isointense on T1-weighted images and iso- to hyperintense or sometimes heterogeneously intense on T2-weighted images. Contrast enhancement generally enhances evenly and often produces a dural tail (Fig. 6) (2).
Fibrous Dysplasia
Fibrous dysplasia is characterized as the replacement of normal cancellous bone with abnormal fibrous tissue (13). On plain radiograph, they appear as ground-glass sclerotic lesions or cystic lesions commonly crossing bony sutures. They may involve multiple calvarial bones (14), tending to cause the outer table to bulge while conserving the shape of the inner table (15). CT scans show a degree of hazy and intradiploic density. On T1-weighted images, they are usually hypointense, but more fibrous areas can be isointense. On T2-weighted images, they show various signals, depending on their cellularity: those that are more fibrous with fewer bony trabeculae and less cellularity exhibit relatively high signal intensities, while more osseous and cellular matrices can show relatively low signal intensities (16). Contrast enhancement produces a variable range of intensities depending on lesion stage; there can be homogeneous, central or peripheral enhancement (Fig. 7).
Lymphoma
Malignant lymphoma may originate in the skull and extend to outside the cranium (17). Presenting as nonspecific osteolytic lesions on plain radiograph, on CT scans they instead appear as extra-intra cranial isodense lesions in the cranial vault or homogenous masses with sharp margins. On MR, most reported cases of skull lymphomas produced isointense signals on pre-contrast T1-weighted images with intense enhancement with contrast. However, MR imaging does not diagnose lymphoma accurately because it can mimic metastatic carcinoma, osteomyelitis, or in some cases, meningioma (Fig. 8) (18).
Desmoplastic Fibroma
Desmoplastic fibroma is a rare benign bone tumor which originates from fibrous tissue, and a majority of cases are seen in those younger than 30 years of age. Desmoplastic fibroma most commonly occurs in the metaphyses of the long bones, the mandible, and the pelvis, whereas the maxilla, calvaria, sternum, and vertebrae are less frequently affected. Simple radiographs show an expansile, osteolytic lesion with a trabeculated or bubbly appearance. At times, the tumor may have a very aggressive radiographic appearance with bone destruction, cortical erosion, or soft-tissue invasion (1920). The dense connective tissue and hypercellular regions have intermediate signal intensity on T1-weighted images and heterogenous signal intensity on T2-weighted images (Fig. 9) (19).
Atretic Meningocehalocele
Atretic cephalocele is composed of dura, fibrous tissue, and dysplastic brain tissue. Oval or elongated defects are observable on plain skull radiographs. On CT scans, a subgaleal soft tissue mass with "spinning top" configuration is seen. On MRI, a subcutaneous scalp mass with intracranial extension through skull and dura may be seen as having heterogeneous signals on T1-weighted images and high signals on T2-weighted images and heterogeneous enhancement after contrast injection. On MR venography, a vertically positioned straight sinus equivalent (persistent falcine vein) is seen (Fig. 10) (21).
Gorham Disease
Gorham disease is an intraosseous neoplastic proliferating disease of hemangiomatous or lymphagiomatous tissue with progressive massive osteolysis. The first stage involves vascular proliferation in connective tissue; in the second stage, fibrous tissue replaces the absorbed bone without regeneration of the bone matrix. On CT scans, radiolucent foci in the intramedullary or subcortical regions are seen and the gradual disappearance of bone may be apparent. MR imaging of Gorham disease involving the calvaria has not been widely reported, but a reticular pattern on a contrast enhanced fat-suppressed T1-weighted image was reported (16).
Burr Hole
Burr holes appear as well-defined defects in the inner and outer tables of the skull vault on CT or simple radiograph. On contrast-enhanced MR images, the margins of the burr hole usually show enhancement, and in some cases, diffuse enhancement with a filling of the plunge defect may be seen. Defects caused by plunging may show high signal intensity on T2-weighted images, which is referred to as a "mushroom sign" (22).
Others
Skull Osteosarcoma
Skull osteosarcomas show nonspecific radiological features, for example, they can be either osteolytic, osteoblastic, or mixed in involvement pattern. However, spicular calcification tends to be seen, and a sun burst appearance exists in 25% to 31% of cases (23). Bone destruction and mineralization of the tumors may indicate an osteogenic sarcoma (24).
Osteomyelitis
Osteomyelitis of the calvarium may occur as a consequence of trauma or as a complication of sinus sepsis. Pus in the bone can spread either into the cranium or outward into subgaleal or subcutaneous planes where it can form abscesses, visible as osteolytic lesions on CT (25).
Arachnoid Granulation
Arachnoid granulations usually present as sharply marginated, lucent, occipital bone lesions adjacent to the transverse sinus. They generally appear as hypointense or isointense relative to the brain parenchyma on T1-weighted images and hyperintense on T2-weighted images and show minimal heterogeneous contrast enhancement (2627).
Neurofibromatosis Type 1
Neurofibromatosis type 1 is a multisystem neurocutaneous disorder that is one of the most common inherited autosomal dominant central nervous system disorders. The radiographic spectrum includes focal areas of abnormal signal intensity in deep grey or white matter, optic nerve glioma, progressive sphenoid wing dysplasia, lambdoid suture defects, dural calcification at the vertex, buphthalmos, and in rare cases, the Moyamoya phenomenon (28).
Focalized or Generalized Thickening of the Calvarium
Osteoblastic Metastasis
Osteoblastic metastases arise from hematogenous spread from primary cancers. In such instances, they are often seen without benign sclerotic borders. On CT scans, metastatic lesions are usually seen as enhancing masses centered in bone with osseous destruction and most are lytic, though a few are sclerotic (e.g., prostate lesions). Osteoblastic metastases appear as hypointense lesions on both T1-weighted and T2-weighted images without significant enhancement and appear positive on DWI (229).
Osteoma
Osteomas are benign, slow-growing tumors usually found incidentally (30). They are the most common benign osseous tumors in the calvarium, and are mainly found in the outer table of the skull (31). They appear as dense oval lesions on radiographs. On CT images, they appear as very hyperdense sclerotic masses with clear-cut outlines that grow from, and attach to, the external aspect of the cortical bone. They are homogeneously hypointense on T1-weighted images, heterogeneously hypointense on T2-weighted images, and do not show contrast enhancement (2).
Fibrous Dysplasia
Fibrous dysplasia can be seen as calvarial thickening because it tends to cause the outer table to bulge while conserving the shape of the inner table (15).
Meningioma
Usually benign, meningiomas arising from the dura can cause hyperostosis. On plain radiograph and CT, 75% of cases appear as round or smoothly lobulated masses that are hyperdense compared to the cerebral cortex. 25% of cases demonstrate calcification. Hyperostosis on bone algorithm CT is often seen (32).
Acromegaly
Growth hormone hypersecretion can manifest as generalized thickening of the skull. Bony abnormalities associated with growth hormone include sella turcica alterations, prominence and enlargement of frontal and maxillary sinuses, excessive pneumatization of the mastoids, prominence of the occipital protuberance, thickening or, less commonly, thinning of the cranial vault, enlargement and elongation of the mandible, and widening of the mandibular angle (32).
Others
Shunted Hydrocephalus
Chronic intracranial hypotension or prolonged ventricular shunting for hydrocephalus can cause diffuse thickening of all bones of the neurocranial vault. This happens because outward pressure needed to expand the cranium is missing, so the inner table of the skull bone grows instead. On simple radiographs and CT scans, the entire cranial vault thickening can be seen (33).
Dilantin Therapy
Dilatin (Diphenylhydantoin) is widely used for the management of patients with epileptic convulsions. Dilatin has recently been shown to stimulate osteoblast proliferation in approximately 34% of patients. The degree of skull thickening is correlated with frontal bossing and degree of facial coarsening (34). The increase in the thickness of the calvarium is mainly presented in the diploic space (35).
Paget Disease
Paget disease, also known as osteitis deformans, can cause chronic metabolic skeletal disorders (2) characterized by bony expansion with variable destruction with or without sclerosis. The characteristics of CT and MR are a loss of normal trabeculae from lysis, a disorganized pattern of trabecular thickening, and, finally, sclerosis when the disease is in the blastic phase. Since a majority of cases are seen in the mixed phase, the yellow marrow signal intensity is maintained regardless of the MR sequence (3637).
Chronic Hemolytic Anemia
Patients with hemolytic anemia have red marrow hyperplasia, causing the widening of the diploic space; the outer table thins or is completely obliterated. Before diploic widening, a coarse granular or stippled pattern can be seen in the upper parietal region. When the hyperplastic marrow perforates or destroys the outer table, new bony spicules perpendicular to the inner table are seen as "hair-on-end" signs (38).
Chronic Calcific Cephalhematoma
Cephalhematoma that is not absorbed within a month begins to ossify where the periosteum is lifted and the ossification gradually covers the surface of the hematoma. The thick band-like ossification mimics doubling of the skull, so it is referred to as a "double skull sign" (39). On CT and radiograph, it appears as a uniform, densely calcified mass located immediately adjacent to the outer table, within the periosteum (1).
Hyperostosis Frontalis Interna
Hyperostosis frontalis interna is a benign condition which thickens the inner table of the frontal bone. Though the etiology is not clearly known, estrogen signaling is thought to be involved. The hyperostotic bone tends to be less dense on simple radiographs or on CT than are normal cortical bones (4041).
Focal or Generalized Thinning of the Calvarium
Prominent Convolutional Marking (Copper-Beaten Skull)
Prominent convolutional marking is widely considered to be a reflection of normal brain growth. The growing brain exerts a continuous pulsatile pressure on the cranium, producing a gyral pattern on plain radiographs which is known as the copper-beaten pattern (42).
Craniosynostosis
Craniosynostosis is a rare, complex condition defined as a premature fusion of one or more of the cranial sutures (43). Primary craniosynostosis is due to a developmental error during embryogenesis, while secondary craniosynostosis is due to mechanical or metabolic causes (44). In plain radiographs, perisutural sclerosis, localized breaking, bony bridging, and absence of the suture are primary signs of craniosynostosis. When raised intracranial pressure is maintained over long, fingerprinting and copper beating can be seen (45).
Lacunar Skull
Lacunar skull is characterized as a dysplasia of the membranous bone caused by mesenchymal abnormality and is associated with neural tube defects, especially myelomeningocele with Chiari II malformation. It is seen as a well-defined lucent lesion (having a scooped-out appearance) which corresponds to the nonossified fibrous bone (32).
Long-Standing Hydrocephalus
Regardless of the cause of hydrocephalus, increased intracranial pressure may result in diffuse calvarial thinning with or without deformity when it is not treated properly (33).
Normal Parietal Thinning
Parietal thinning is an uncommon condition which can be caused by either non-progressive congenital dysplasia of the dipole or acquired and progressive diseases such as tumors, diabetes, long-standing steroid therapy, or osteoporosis. The bilateral parietal bones show symmetrical thinning (involving the outer tables and diploe) with a scalloped appearance while the inner table is usually intact (4647).
Secondary Thinning due to Benign Tumors
Benign tumors or slow growing cysts can result in overlying skull thinning because of a chronic pressure effect. Smooth-margined calvarial thinning without periosteal reaction or new bone formation suggests that the underlying lesion is benign.
Parry Romberg Syndrome
Parry Romberg syndrome is rare neurocutaneous disorder also known as progressive hemifacial atrophy. One side of the face, including the skin, subcutaneous tissue, muscles, cartilage, and underlying bony structures, becomes slowly and progressively atrophic. Radiologic findings include bone and soft-tissue atrophy of varying degrees, which do not cross the midline (48).
CONCLUSION
Calvarial lesions vary from clinically insignificant lesions to life-threatening lesions such as bone metastases. While bony lesions of the calvarium are easily identified using brain CTs, bone marrow lesions can be visualized better on brain MRIs than on brain CTs. Diffusion-weighted MRI is helpful in detection and diagnosis of bone marrow lesions. The categorical imaging approach presented here will be helpful in narrowing the list of possible diagnoses of calvarial lesions.








 XML Download
XML Download