

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The use of breast magnetic resonance imaging (MRI) is increasing for screening and diagnosis of breast cancer. MRI has greater sensitivity than other imaging modalities for the screening of women at higher risk of breast cancer, with more than half of lesions only detected on MRI (12). MRI can identify primary cancer in suspected occult breast cancer patients (3). In addition, breast MRI most accurately depicts the extent of breast cancer (456). Although the clinical relevance of additional lesions is still controversial, preoperative MRI identifies more synchronous, ipsilateral or contralateral breast cancers than mammography and ultrasound (789).
However, breast MRI has limited specificity (10). If a suspicious lesion is detected, biopsy is mandatory to avoid unnecessary surgery. In addition, biopsy under MRI guidance is required for suspected occult lesions on mammography or ultrasound. The American College of Radiology requires performance of MRI-guided intervention or contact with available referral site when performing breast MRI (11). The MRI guideline of the European Society of Breast Imaging also emphasizes the necessity of offering MRI-guided intervention at a site performing breast MRI (12). The number of medical centers providing breast MRI is growing in Korea, and more MRI-guided breast biopsies are required. However, few reports describe MRI-guided breast biopsy in Korea (1314). In this article, we describe preprocedural considerations and technique, and correlation of radiologic and pathologic findings in MRI-guided breast biopsy.
PREPROCEDURAL CONSIDERATIONS FOR MRI-GUIDED BREAST BIOPSY
Second-Look Studies
Second-look studies should be considered for all women with suspicious lesions on MRI. If the lesion is delineated with mammography or ultrasound, biopsy under imaging guidance using these modalities is preferred. MRI-guided biopsy is more expensive and difficult for the patient. However, the reported correlation rate of second-look ultrasound ranges from 23–57%; MRI-only lesions require an MRI-guided biopsy (15161718).
Patient Preparation
Informed consent should be obtained before the biopsy. Patients with a known contraindication for MRI or gadolinium administration should not have an MRI-guided biopsy. Patients with allergy to gadolinium or local anesthetics are also not suitable. Bleeding risk due to use of aspirin or anticoagulants or an underlying coagulation disorder is a relative contraindication for biopsy, requiring careful consideration of the risks and benefits. The patient should be able to remain prone during the biopsy for a minimum of 60 minutes. The possibility of a nonvisualized target lesion should be discussed with the patient. Even with successful visualization, the cancellation of a biopsy is sometimes necessary because of unforeseen safety issues. Complications such as hematoma, infection, and skin injury should also be discussed with the patient. For patients with breast implants, rupture is a possible complication of the biopsy.
MRI-GUIDED BREAST BIOPSY PROCEDURE
Table 1 summarizes the biopsy procedure.
Positioning
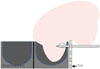
The patient lies in a prone position, and a dedicated interventional breast coil is used. Either a grid or a pillar and post system is generally used. We focus on the grid system, which is most widely used (Fig. 1). The breast within the coil is compressed by the grid. Compression pressure is adjusted for stable immobilization while preserving blood flow. The approach to a posterior mass is often difficult, requiring that sufficient breast tissue be contained in the grid to maintain distance from the chest wall. Fixing a fiducial marker to the grid enhances target localization.
Equipment
MRI-guided vacuum assisted biopsy (VAB) has advantages over standard core biopsy. The larger core size results in decreased sampling error and compensates for tissue shifting during needle placement (19). The European consensus group recommend a minimum 11-gauge probe size (20). The MRI-guided biopsy kit consists of an introducer stylet, obturator, introducer sheath, and needle guide. The needle guide, a cube-shaped plastic block with multiple holes for the biopsy device (Fig. 2), maintains the VAB device perpendicular to the grid.
Image Acquisition and Lesion Localization
Fig. 3 shows the MRI-guided biopsy sequence. A precontrast T1-weighted fat-saturation sequence is obtained to determine whether the target lesion is within the grid. If the target lesion is too small for detection on the precontrast image, anatomic landmarks are helpful for identification. If the precontrast image indicates that the lesion is inaccessible, the patient's position should be adjusted. After planning the proper approach route, postcontrast T1-weighted fat-saturation images are obtained. The thickness and in-plane resolution, which are similar to that of diagnostic imaging for accurate needle positioning, make localization easier. Sagittal and axial plane images are obtained. Alternatively, axial or sagittal plane images with perpendicular reconstruction can be used for lesion localization depending on the physician's preference. The entry site on the grid and depth from the skin to the lesion are measured using the fiducial marker as a reference. A worksheet provided by the manufacturer is helpful in manual localization (Fig. 4). The thickness of the needle guide should be included in the calculation. A computer-assisted diagnostic system that improves accuracy and speed of the procedure is also commercially available. About 8–13% of MRIguided biopsy target lesions are not visible at the time of biopsy (212223). If the target is not visible on the first postcontrast image, it is sometimes identified on a delayed image. Overpressure by the grid may interfere with breast perfusion and should be checked. A subtraction image also aids in lesion identification (Fig. 5). If the target lesion is still not visible, short-term followup is recommended at about 6 months.
Biopsy Procedure
After standard skin preparation, local anesthesia is administered. A small nick in the skin facilitates smooth entry by the VAB device. The introducer stylet within its sheath is inserted through the needle guide to the measured depth. A twisting motion is helpful to avoid skin tenting and tissue displacement. The stylet is removed and replaced by the obturator. T1-weighted fat-saturation images are then obtained to confirm the depth and position of the introducer (2425). In the case of insufficient depth, the introducer sheath can be advanced after reinsertion of the stylet; if advanced past the target lesion, the introducer is gradually withdrawn. In general, the optimal position is in the center of the target. Directional sampling can be performed with a peripheral location of the needle. When the introducer position is verified as correct, the obturator is exchanged with a VAB device. The European consensus group recommends no less than 24 samples for an 11-gauge or equivalent volume if a larger probe is used (20). Liberman (26) reported that an 11-gauge VAB device collects 100 mg, and a 9-gauge VAB device collects 200 mg. T1-weighted fat-saturation images are obtained immediately after the biopsy to evaluate adequacy. Image assessment can be difficult due to contrast washout, background enhancement, hemorrhage, and air, but careful review using anatomic landmarks improves the evaluation accuracy. An additional biopsy can be performed if the target sample is insufficient. Once the target sampling is acceptable, marker clip should be placed through the introducer sheath. A post-clip-insertion image may be obtained with MRI or mammography. The importance of marker clip insertion should never be underestimated. The marker clip facilitates mammographic or ultrasound-guided localization in place of MRI-guided localization for subsequent excisional biopsy. Moreover, if the entire target lesion is removed by VAB, the marker clip is the only way to identify the biopsy site. The breast is compressed for at least 15 minutes after the biopsy.
Complications and Management
Major complications requiring surgical intervention seldom occur with MRI-guided biopsy. Complication rates are less than 5%. Bleeding and hematoma formation are most common, and can be controlled by compression. Other rare complications are skin laceration, vasovagal syncope, and infection. Termination of the procedure due to a complication is rare (1927282930313233343536).
CHALLENGING SITUATIONS AND TROUBLESHOOTING
Targeting deep-seated lesions is prone to chest wall injury. To avoid this, traction on the breast tissue as much as possible, coil padding removal, and biopsy toward the anterior side are some solutions (33). A posteromedial target location is the most difficult to access. If the patient is small, a lateral approach from the contralateral opening of the breast coil can make a deep posterior location more accessible (Fig. 6). A thin breast is another challenge for MRI-guided biopsy. A generous amount of anesthetic agent helps to increase breast thickness, and a reverse compression paddle is also useful (2437). VAB devices with smaller apertures or blunt tips can be used for targets in thin breasts and also those near the skin (Table 2).
RADIOLOGIC-PATHOLOGIC CORRELATION
As with all other image-guided biopsy techniques, MRI-guided biopsy results should be evaluated for radiologic-pathologic concordance. MRI-guided biopsy has no corresponding evaluation method such as specimen imaging in stereotactic biopsy or real-time monitoring in ultrasound-guided biopsy; therefore, radiologic-pathologic concordance requires caution. The positive predictive value of a lesion detected by MRI with subsequent MRI-guided biopsy is 16–61%; a radiologist should be aware that for radiologic-pathologic correlation, the positive predictive value is affected by the prevalence of breast cancer in a patient population (19303336383940). A six-month follow-up is recommended for a benign concordant biopsy result (41). The rate of radiology-pathology discordance is not high (0% to 10.7%); but the mean proportion of malignancies in discordant cases is 37.5%, and surgical excision is recommended for discordant lesions (Table 3) (19293034363839).
The atypical ductal hyperplasia (ADH) upgrade rate at surgery is reportedly 25–38% (193038404243). In ductal carcinoma in situ (DCIS), the upgrade rate ranges from 5–24% (19303844). The underestimation rates for ADH and DCIS on MRI-guided biopsy are slightly higher than those for stereotactic biopsy (21% and 11%, respectively) (4546) or ultrasoundguided biopsy (23.3% and 13.8%, respectively) (47). Atypical lobular hyperplasia and lobular carcinoma in situ also have a high upgrade rate (27%) (40). Despite a limited number of studies in the underestimation rate for other high-risk lesions such as radial scars and papillomas, surgical excision for all such lesions using MRI-guided biopsy is recommended (303840).
CONCLUSION
Breast MRI is an important screening and diagnostic tool, but the limited specificity requires biopsy confirmation. MRIonly lesions that are occult on mammography and ultrasound require routine evaluation by MRI-guided biopsy. Radiologists who perform the procedure understand best the indications, preprocedural considerations, imaging protocols, biopsy techniques, and possible complications of MRI-guided VAB. Patients should be informed about the demanding nature of the procedure due to prolonged immobilization, the possibility of cancellation of the procedure, and the need for imaging follow-up despite a benign biopsy result. Appropriate patient management based on radiologic-pathologic correlation is emphasized.








 XML Download
XML Download