

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Video-assisted thoracic surgery (VATS) is a minimally invasive technique commonly used worldwide for biopsy or resection of pulmonary lesions. Although VATS procedures are considered safe and effective, they have potential complications such as prolonged air leak, bleeding, infection, and port site metastasis. Port site metastasis is a rare complication after VATS for a malignancy, with a few reports of mesothelioma cases and others (1234). However, to our knowledge, it has not been reported in a breast cancer patient in the English literature. We reported the first case of iatrogenic port site metastasis in a breast cancer patient who received VATS wedge resection for pulmonary metastasis.
CASE REPORT
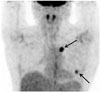
We experienced a case of a 57-year-old woman who had undergone modified radical mastectomy for clinical stage T3N1M0 triple negative subtype invasive ductal carcinoma (IDC) of the right breast. After 2 years, 2 pulmonary metastatic nodules were suspected in her left lung on a surveillance positron emission tomography-computed tomography (PET-CT) scan (Fig. 1). She underwent VATS wedge resection and the lung nodules were pathologically confirmed as metastatic IDC.
Six months after VATS, she presented at our hospital with a small palpable mass on the left breast periphery. Ultrasonography (US) revealed an approximately 2.0 cm sized, circumscribed, round, and complex echoic mass with internal vascularity (on color Doppler US) in the lower outer quadrant periphery of the left breast just beneath the VATS port site scar (Fig. 2). The dif
ferential diagnosis included tumor spread, metachronous or contralateral secondary primary cancer; however, since the mass was detected at the site of the postoperative scar on the first follow-up US after VATS resection with no abnormal uptake on the previous post-op PET-CT taken 4 months prior, the possibility of postoperative organizing hematoma was also considered. Consequently, the lesion was initially rated as category 4a (low suspicion for malignancy) according to the Breast Imaging-Reporting and Data System; and as a precaution, follow up US was decided upon.
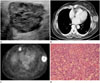
After 6 months, the follow-up US revealed an increase in the mass size (3.8 × 3 × 3.4 cm), as compared to the previous US (Fig. 3A). In addition, a consecutively performed contrast enhanced CT revealed a necrotic rim enhancing lobulated mass and PET-CT scan showed hot uptake with maximum standardized uptake value of 5.0 at the previous VATS port site (Fig. 3B, C). Subsequent excisional biopsy was confirmed histopathologically as metastatic IDC consistent with primary triple negative breast cancer (Fig. 3D). Despite complete resection of the port site metastatic mass and chemotherapy, recurrent pulmonary metastasis and pleural seeding developed and the patient expired 2 years later.
DISCUSSION
VATS is currently a routinely performed procedure for the management of metastatic lung tumor, especially when the lesion is located peripherally and is small in size and number. Compared with open thoracotomy, VATS provides many advantages: smaller incisions, better visualization of the pleural cavity, less postoperative pain, less surgical morbidity, shorter length of hospitalization, fewer adhesions, shorter interval between surgery, and adjuvant therapy with better treatment compliance. But there are also complications such as prolonged air leak, bleeding, postoperative wound infections, and metastasis at the port site (5). Port site metastasis is a rare complication of VATS for malignancy with an overall incidence of 0.12–0.57% (56). The port site metastasis is an indicator of multifocal disease with poor prognosis and increasing mortality (6). While the mechanism of port site metastasis has not been clarified, tumor implantation in the port wound is considered as the most likely cause (1). There are only a few reported cases of port site metastasis after VATS procedures for pulmonary malignancies due to pulmonary adenocarcinoma, mesothelioma, metastatic colorectal carcinoma, metastatic endometrial carcinoma, metastatic medullary thyroid carcinoma, metastatic melanoma (1234).
However, to our best knowledge, port site metastasis of breast cancer has not yet been reported in the English literature. In general, for newly developed masses in the contralateral breast after mastectomy for breast cancer, the first differential diagnosis is synchronous or metachronous breast cancer, or second primary breast cancer. This is because women with unilateral breast cancer are at an increased risk for the development of contralateral breast cancers, with a 1–5% incidence of synchronous cancer and a 3–13% incidence of metachronous cancer (78). Also, the risk of developing a second primary breast cancer for women with unilateral breast cancer is 2–6 times higher than the general population (9). In our case, a palpable mass developed at the port site, 6 months after VATS, which was detected at the first postoperative follow-up US, therefore, differential diagnosis included not only contralateral metachronous or second primary breast cancer, but also postoperative organizing hematoma. All of the above lesions can be seen as growing masses, tend to have well-demarcated contours, and can demonstrate similar sonographic findings as complex echoic lesions. However, organizing hematoma usually shows no flow on color Doppler US.
In conclusion, this was a rare case of port site metastasis after resection of pulmonary metastasis from breast cancer by VATS. Thus, radiologists should consider port site metastasis in the differential diagnosis in cases of newly developed masses at the port site following VATS for pulmonary metastasis. Furthermore, clinicians should not hesitate to perform a biopsy for early detection and diagnosis of the potentially fatal complication of port site metastasis.

 XML Download
XML Download