

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tuberculous infection is one of the manifestations of skeletal involvement of human immunodeficiency virus (HIV)-infected patients that most commonly involves the spine (1). The radiologic features reported in the literature are characterized by destruction of the vertebral body, subligamentous extension, frequent paravertebral abscess formation and late involvement of the disk space. Usually, these lesions are hypointense on T1-weighted imaging and heterogeneously hyperintense on T2-weighted imaging on magnetic resonance imaging (MRI) (23). Herein, we reported a case of a 25-year-old male who was confirmed with spinal tuberculosis by computed tomography (CT)-guided biopsy without the appearance of the abovementioned findings on abdominal CT and spine MRI. To our knowledge, these results are not reported previously in the English-medical literature; herein, we reported this feature as one of the manifestations of tuberculous spondylitis.
CASE REPORT
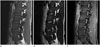
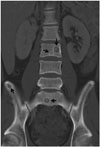
A 25-year-old male visited the outpatient clinic of the infection division of the internal medicine department of our hospital with a complaint of mild abdominal pain of 1 week duration and a cough and purulent sputum. He had started antituberculosis medication 2 months prior because of cervical tuberculous lymphadenitis. He was a known HIV carrier for at least 6 years, but had not received antiretroviral therapy. On physical examination, he showed no abdominal tenderness. He was admitted to the hospital for further evaluation. He was started on antiviral agent therapy immediately. A blood test 2 months prior to admission showed a CD4 cell count of 199 cells/µL [< 200 cells/µL is diagnostic for acquired immune deficiency syndrome (AIDS)]. At the time of admission, his blood test also showed elevated liver enzymes and C-reactive protein; therefore, abdominal CT was performed. Abdominal CT showed no cause of the abdominal pain and elevated liver enzymes; however, incidentally, multiple disseminated osteolytic lesions were noted in the thoracic, lumbar, and sacral vertebrae, as well as in both ilii (Fig. 1). These lesions were well-demarcated and ovoid in shape. Bacillary angiomatosis, Kaposi's sarcoma and spinal tuberculosis were the differential diagnosis of the lesions. The patient underwent lumbar spine MRI. On T1-weighted imaging, the whole spine showed decreased signal intensity. Multiple small, round-to-ovoid lesions were observed in the lower thoracic, lumbar, and sacrum vertebrae, as well as in both ilii. On T1- and T2-weighted imaging with or without fat saturation, these lesions showed isointense signal intensity with a peripheral hyperintense rim that had a target-like appearance. Gadolinium-enhanced T1-weighted imaging showed peripheral rim enhancement of the lesions (Fig. 2). No paravertebral soft tissue mass or abscess was demonstrated. The differential diagnosis on imaging included hematogenously spread lesions, such as tuberculosis and tumor metastases. We performed CT-guided biopsy at the third lumbar vertebral body targeting an ovoid osteolytic lesion on the left side of the vertebral body; and a core of the specimen was acquired. The pathologic examination revealed caseous necrosis on hematoxylin-eosin staining and acid-fast bacilli by the Ziehl-Nielsen method. Polymerase chain reaction showed positivity for Mycobacterium tuberculosis. Focal viable bone marrow tissue adjacent to the lesion revealed a mild increment of histiocytes and eosinophils that was consistent with reactive proliferation (Fig. 3). Based on the pathologic diagnosis of spinal tuberculosis, the patient was suspected of having immune reconstitution inflammatory syndrome, which is a paradoxical reaction following antiretroviral therapy due to the regained host capacity to mount an inflammatory response. He did not undergo additional spine MRI or CT; however, chest CT performed 2 months later showed multiple disseminated osteolytic lesions on the thoracic spine, identical to those of the lumbar spine. Miliary tuberculosis of the lung and splenic tuberculosis developed, and antituberculosis medication was continued (Fig. 4). Ten months later, he underwent abdominal CT again for the evaluation of splenic tuberculosis. The osteolytic lesions in the lower thoracic and lumbar spine, sacrum, and both ilii were unchanged since the last study and not normalized even after continuous antituberculosis medication (Fig. 5).
DISCUSSION
Musculoskeletal manifestations in HIV-positive patients show a wide spectrum of disease, including infectious, inflammatory, and neoplastic disease, anemia, osteonecrosis, or rhabdomyolysis. Osteomyelitis is one of the infectious diseases that may occur and is usually associated with CD4 cell counts of < 250/µL (1). Particularly, tuberculosis infection and bacillary angiomatosis are 2 specific forms of osteomyelitis that are reported in HIV-infected patients. Although tuberculosis affects mostly the pulmonary system, musculoskeletal involvement is the fourth most common type of extrapulmonary tuberculosis and accounts for up to 3% of tuberculosis infections in HIV-infected patients. Skeletal involvement is primarily by the hematogenous route. Unlike the typical solitary tuberculosis lesions in immunocompetent patients, HIV-infected patients have multicentric lesions in ~30% of cases (12).
The spine is the most common site of skeletal tuberculosis, which is also known as Pott's disease. Spinal tuberculosis reportedly occurs in up to 50–60% of skeletal tuberculosis. The lower thoracic or upper lumbar vertebrae are the most frequently affected areas (13). The infection is spread by perivertebral arterial or venous plexi and typically begins in the anterior aspect of the vertebral body and extends subligamentously to the vertebral column, sparing the posterior column. Subsequent paraspinal soft tissue involvement with abscess formation is also noted; finally, the intervertebral disk becomes involved (13).
Radiography of tuberculous spondylitis may demonstrate erosion of the anterior vertebral body, loss of vertebral height, indistinct end plates and paravertebral mass. No pathognomonic signs distinguish tuberculous spondylitis from pyogenic spondylitis. On MRI, T1-weighted images of the affected vertebrae show decreased signal intensity, and T2-weighted images show a heterogeneously increased signal. Gadolinium-enhanced T1-weighted images show heterogeneous enhancement of the lesion and peripheral rim enhancement of paravertebral or epidural abscesses, which are diagnostic findings. Chronic tuberculous spondylitis shows variable signal intensity; T1-weighted images may show increased or decreased signal intensity. Hyperintense signal intensity on T1-weighted images of the involved vertebrae that normalizes with treatment is specific to chronic tuberculous spondylitis (34).
The differential diagnosis of tuberculous spondylitis includes other infectious and neoplastic diseases. Osteolytic lesions are also reported in bacillary angiomatosis, an unusual form of osteomyelitis caused by Bartonella species. Bacillary angiomatosis shows well-defined, nonsclerotic, lytic vertebral lesions with periosteal reaction on CT. MRI shows low signal intensity on T1- and high signal intensity on T2-weighted imaging (2). Kaposi's sarcoma presents as multiple osteolytic foci on the chest wall, pelvis, spine or shoulders, and periostitis is uncommon. MRI may show an isointense signal on T1-weighted imaging and a hyperintense signal on T2-weighted imaging with intense enhancement after gadolinium injection. The imaging findings of bacillary angiomatosis or Kaposi's sarcoma can be difficult to distinguish from those of tuberculosis (5). However, bacillary angiomatosis and Kaposi's sarcoma show characteristic skin lesions in most cases that are not found in tuberculosis (2). Metastatic disease usually shows decreased signal intensity on T1-weighted images and increased signal intensity on T2-weighted images on MRI. However, our patient was a young immunocompromised male, and no evidence of primary malignancy was found on abdominal and chest CT, indicating a low probability of spinal metastasis.
In HIV-infected patients, the vertebral marrow may show uniformly decreased signal intensity on T1-weighted imaging and increased signal intensity on T2-weighted imaging, as in our patient. These features are known to be correlated with anemia associated with chronic disease, in which impaired release of iron from macrophages leads to accumulation of iron within the bone marrow (2).
Currently, we have no information concerning multiple well-defined, target-like appearances that occur in spinal tuberculosis but not in other infectious diseases or malignancy involving the axial skeleton. Some well-defined lesions include bacillary angiomatosis, but target-like appearances are not typical manifestations. There are some reports of unusual image findings of tuberculosis spondylitis, such as solitary or multiple vertebral lesions without disk involvement and paraspinal abscess (6). However, to our knowledge, isointense signal intensity with peripheral rim enhancement has not been reported previously for tuberculosis spondylitis in the English medical literature. These unusual target like findings reflect disseminated tuberculosis, which consist of central caseous necrotic zone and peripheral active inflammatory zone. The lower CD4 cell count level could possibly contribute to this atypical, extrapulmonary and disseminated disease. However, its relationship with AIDS remains unclear.



 XML Download
XML Download